World Journal of Emergency Medicine ›› 2024, Vol. 15 ›› Issue (3): 175-180.doi: 10.5847/wjem.j.1920-8642.2024.032
• Original Articles • Previous Articles Next Articles
Yedalm Yoo, Shin Ahn( ), Bora Chae, Won Young Kim
), Bora Chae, Won Young Kim
Received:2023-06-20
Accepted:2023-11-16
Online:2024-05-15
Published:2024-05-01
Contact:
Shin Ahn, Email: Yedalm Yoo, Shin Ahn, Bora Chae, Won Young Kim. Performance of the EDACS-ADP incorporating high-sensitivity troponin assay: Do components of major adverse cardiac events matter?[J]. World Journal of Emergency Medicine, 2024, 15(3): 175-180.
Add to citation manager EndNote|Ris|BibTeX
URL: http://wjem.com.cn/EN/10.5847/wjem.j.1920-8642.2024.032
Table 1.
Baseline characteristics
| Parameters | All patients (n=1,304) | MACE I a (+) (n=410) | MACE I a (-) (n=894) | P-value |
|---|---|---|---|---|
| Age, years, mean±SD | 62.7±15.2 | 68.8±11.7 | 59.9±15.8 | <0.001 |
| Sex: Male, n (%) | 790 (60.6) | 289 (70.5) | 501 (56.0) | <0.001 |
| Cardiovascular risk factors, n (%) | ||||
| Hypertension | 621 (47.6) | 245 (59.8) | 376 (42.1) | <0.001 |
| Diabetes | 294 (22.5) | 144 (35.1) | 150 (16.8) | <0.001 |
| Dyslipidemia | 323 (24.8) | 113 (27.6) | 210 (23.5) | 0.128 |
| Family history of CAD | 130 (10.0) | 45 (11.0) | 85 (9.5) | 0.426 |
| Cerebrovascular disease | 97 (7.4) | 35 (8.5) | 62 (6.9) | 0.308 |
| Smoking: current or cessation <3 months | 146 (11.2) | 70 (17.1) | 76 (8.5) | <0.001 |
| Obesity (BMI ≥30 kg/m2) | 62 (4.8) | 18 (4.4) | 44 (4.9) | 0.780 |
| History of CAD, n (%) | ||||
| Acute myocardial infarction | 90 (6.9) | 43 (10.5) | 47 (5.3) | 0.001 |
| Percutaneous coronary intervention | 322 (24.7) | 162 (39.5) | 160 (17.9) | <0.001 |
| Coronary artery bypass graft | 53 (4.1) | 25 (6.1) | 28 (3.1) | 0.015 |
| Symptoms and signs, n (%) | ||||
| Diaphoresis | 253 (19.4) | 132 (32.2) | 121 (13.5) | <0.001 |
| Radiation to the arm or shoulder | 310 (23.8) | 140 (34.1) | 170 (19.0) | <0.001 |
| Pain occurred or worsened with inspiration | 91 (7.0) | 5 (1.2) | 86 (9.6) | <0.001 |
| Pain reproduced by palpation | 22 (1.7) | 0 (0.0) | 22 (2.5) | <0.001 |
| Troponin I, ng/mL, median (IQR) | ||||
| Initial (0 h) | 0.01 (0.01-0.05) | 0.04 (0.01-0.31) | 0.01 (0.01-0.02) | <0.001 |
| Follow-up (2 h) | 0.01 (0.01-0.09) | 0.08 (0.01-1.26) | 0.01 (0.00-0.02) | <0.001 |
| New ischemia on ECG, n (%) | 356 (27.3) | 201 (49.0) | 155 (17.3) | <0.001 |
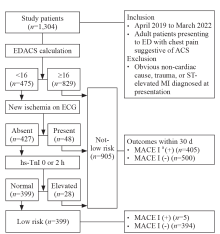
Figure 1.
Flow diagram of patients in the study. EDACS: Emergency Department Assessment of Chest pain Score; ED: emergency department; ACS: acute coronary syndrome; MI: myocardial infarction; ECG: electrocardiography; hs-TnI: high-sensitivity troponin I; MACE: major adverse cardiac event; a: acute myocardial infarction, emergency revascularization, cardiovascular death, ventricular arrhythmia, cardiac arrest, cardiogenic shock, and unstable angina.
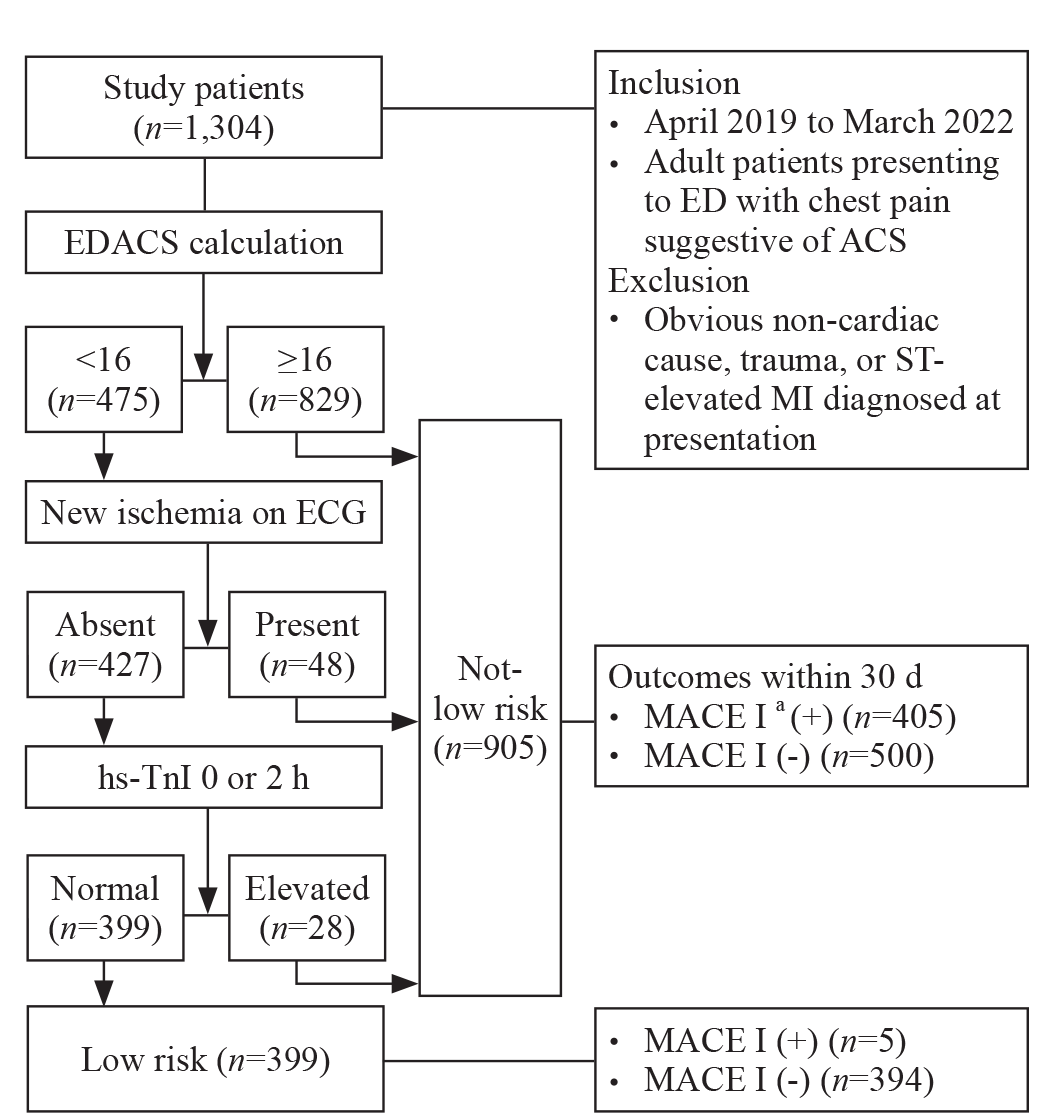

Figure 2.
Prevalence of MACE according to EDACS and EDACS-ADP. MACE: major adverse cardiac event; EDACS: Emergency Department Assessment of Chest pain Score; ADP: accelerated diagnostic protocol. a: MACE I: MACE II + unstable angina; b: MACE II: acute myocardial infarction, emergency revascularization, cardiovascular death, ventricular arrhythmia, cardiac arrest, and cardiogenic shock.
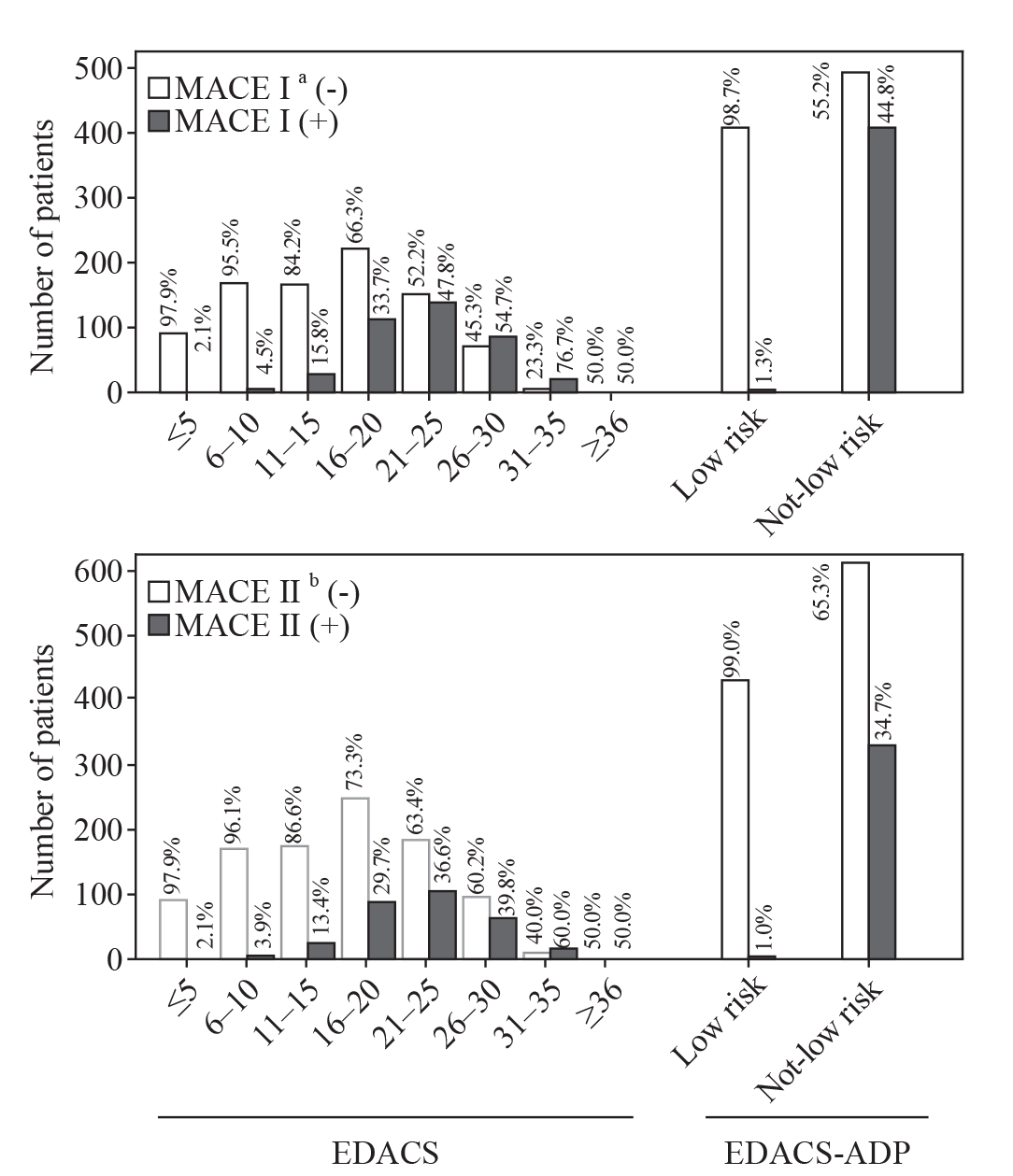
Table 2.
Comparison of EDACS, ECG with hs-TnI, and EDACS-ADP
| Groups | EDACS | ECG with hs-TnI | EDACS-ADP |
|---|---|---|---|
| MACE I a (+) (n=410, 31.4%) | |||
| Not-low risk, n (%) | 368 (44.4) | 273 (59.5) | 405 (44.8) |
| Low risk, n (%) | 42 (8.8) | 137 (16.2) | 5 (1.3) |
| Sensitivity b | 89.8 (86.4-92.5) | 66.6 (61.8-71.1) | 98.8 (97.2-99.6) |
| MACE I a (-) (n=894, 68.6%) | |||
| Not-low risk, n (%) | 461 (55.6) | 186 (40.5) | 500 (55.2) |
| Low risk, n (%) | 433 (91.2) | 708 (83.8) | 394 (98.7) |
| Specificity b | 48.4 (45.1-51.8) | 79.2 (76.4-81.8) | 44.1 (40.8-47.4) |
| Positive predictive value b | 44.4 (42.6-46.2) | 59.5 (55.9-62.9) | 44.8 (43.3-46.2) |
| Negative predictive value b | 91.2 (88.5-93.3) | 83.8 (81.8-85.6) | 98.7 (97.0-99.5) |
| MACE II c (+) (n=318, 24.4%) | |||
| Not-low risk, n (%) | 282 (34.0) | 232 (50.5) | 314 (34.7) |
| Low risk, n (%) | 36 (7.6) | 86 (10.2) | 4 (1.0) |
| Sensitivity b | 88.7 (84.7-91.9) | 73.0 (67.7-77.8) | 98.7 (96.8-99.7) |
| MACE II c (-) (n=986, 75.6%) | |||
| Not-low risk, n (%) | 547 (66.0) | 227 (49.5) | 591 (65.3) |
| Low risk, n (%) | 439 (92.4) | 759 (89.8) | 395 (99.0) |
| Specificity b | 44.5(41.4-47.7) | 77.0 (74.2-80.0) | 40.0 (37.0-43.2) |
| Positive predictive value b | 34.0 (32.5-35.6) | 50.5 (47.2-53.8) | 34.7 (33.5-35.9) |
| Negative predictive value b | 92.4 (89.9-94.3) | 89.8 (88.0-91.4) | 99.0 (97.4-99.6) |
| Rate of low-risk assigned, n (%) b | 475 (36.4, 33.2-39.9) | 845 (64.8, 60.5-69.3) | 399 (30.6, 27.7-33.8) |
| 1 |
van Nieuwkerk JL, van der Linden MC, Verheul RJ, Gaalen MVL, Janmaat M, van der Linden N. The impact of prehospital blood sampling on the emergency department process of patients with chest pain: a pragmatic non-randomized controlled trial. World J Emerg Med. 2023; 14(4):257-64.
doi: 10.5847/wjem.j.1920-8642.2023.054 pmid: 37425086 |
| 2 |
McKenna P, Heslin SM, Viccellio P, Mallon WK, Hernandez C, Morley EJ. Emergency department and hospital crowding: causes, consequences, and cures. Clin Exp Emerg Med. 2019; 6(3):189-95.
doi: 10.15441/ceem.18.022 pmid: 31295991 |
| 3 | Redberg RF. Coronary CT angiography for acute chest pain. N Engl J Med. 2012; 367(4):375-6. |
| 4 |
Than M, Flaws D, Sanders S, Doust J, Glasziou P, Kline J, et al. Development and validation of the Emergency Department Assessment of Chest pain Score and 2 h accelerated diagnostic protocol. Emerg Med Australas. 2014; 26(1):34-44.
doi: 10.1111/1742-6723.12164 pmid: 24428678 |
| 5 | Reichlin T, Hochholzer W, Bassetti S, Steuer S, Stelzig C, Hartwiger S, et al. Early diagnosis of myocardial infarction with sensitive cardiac troponin assays. N Engl J Med. 2009; 361(9):858-67. |
| 6 |
Kim MJ, Ha SO, Park YS, Yi JH, Yang WS, Kim JH. Validation and modification of HEART score components for patients with chest pain in the emergency department. Clin Exp Emerg Med. 2021; 8(4):279-88.
doi: 10.15441/ceem.20.106 pmid: 35000355 |
| 7 | Flaws D, Than M, Scheuermeyer FX, Christenson J, Boychuk B, Greenslade JH, et al. External validation of the Emergency Department Assessment of Chest Score accelerated diagnostic protocol (EDACS-ADP). Emerg Med J. 2016; 33(9):618-25. |
| 8 |
Nilsson T, Johannesson E, Lundager Forberg J, Mokhtari A, Ekelund U. Diagnostic accuracy of the HEART pathway and EDACS-ADP when combined with a 0-hour/1-hour hs-cTnT protocol for assessment of acute chest pain patients. Emerg Med J. 2021; 38(11):808-13.
doi: 10.1136/emermed-2020-210833 pmid: 33837120 |
| 9 |
Kip KE, Hollabaugh K, Marroquin OC, Williams DO. The problem with composite end points in cardiovascular studies: the story of major adverse cardiac events and percutaneous coronary intervention. J Am Coll Cardiol. 2008; 51(7):701-7.
doi: 10.1016/j.jacc.2007.10.034 pmid: 18279733 |
| 10 | Kim RB, Li A, Park KS, Kang YS, Kim JR, Navarese EP, et al. Low-dose aspirin for primary prevention of cardiovascular events comparing East Asians with Westerners: a meta-analysis. JACC Asia. 2023; 3(6):846-62. |
| 11 | Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, et al. Fourth universal definition of myocardial infarction (2018). Circulation. 2018; 138(20):e618-e51. |
| 12 | Collet JP, Thiele H, Barbato E, Barthelemy O, Bauersachs J, Bhatt DL, et al. 2020 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021; 42(14):1289-367. |
| 13 |
Than M, Herbert M, Flaws D, Cullen L, Hess E, Hollander JE, et al. What is an acceptable risk of major adverse cardiac event in chest pain patients soon after discharge from the emergency department?: a clinical survey. Int J Cardiol. 2013; 166(3):752-4.
doi: 10.1016/j.ijcard.2012.09.171 pmid: 23084108 |
| 14 |
Brenner H, Gefeller O. Variation of sensitivity, specificity, likelihood ratios and predictive values with disease prevalence. Stat Med. 1997; 16(9):981-91.
doi: 10.1002/(sici)1097-0258(19970515)16:9<981::aid-sim510>3.0.co;2-n pmid: 9160493 |
| 15 |
Braunwald E, Morrow DA. Unstable angina: is it time for a requiem? Circulation. 2013; 127(24):2452-7.
doi: 10.1161/CIRCULATIONAHA.113.001258 pmid: 23775194 |
| 16 |
Cullen L, Mueller C, Parsonage WA, Wildi K, Greenslade JH, Twerenbold R, et al. Validation of high-sensitivity troponin I in a 2-hour diagnostic strategy to assess 30-day outcomes in emergency department patients with possible acute coronary syndrome. J Am Coll Cardiol. 2013; 62(14):1242-9.
doi: S0735-1097(13)01410-1 pmid: 23583250 |
| [1] | Jonathan Chabon, Jemer Garrido, Deanna Schreiber-Gregory, Jefferson Drapkin, Sergey Motov. Trends in oxycodone and oxycodone-containing analgesics administration for back pain in emergency departments in the USA (2007-2018) [J]. World Journal of Emergency Medicine, 2024, 15(3): 169-174. |
| [2] | Zeyu Yang, Huiruo Liu, Dazhou Lu, Shengchuan Cao, Feng Xu, Chuanbao Li. Effects of high-dose glucose-insulin-potassium on acute coronary syndrome patients receiving reperfusion therapy: a meta-analysis [J]. World Journal of Emergency Medicine, 2024, 15(3): 181-189. |
| [3] | Won Jae Yoo, Shin Ahn, Bora Chae, Won Young Kim. Computed tomography coronary angiography after excluding myocardial infarction: high-sensitivity troponin versus risk score-guided approach [J]. World Journal of Emergency Medicine, 2023, 14(6): 428-433. |
| [4] | Diogo de Almeida Fernandes, Guilherme de Freitas Camões, Diana Ferreira, Carolina Queijo, Carlos Fontes-Ribeiro, Lino Gonçalves, Rui Pina, Natália António. Prevalence and risk factors for acquired long QT syndrome in the emergency department: a retrospective observational study [J]. World Journal of Emergency Medicine, 2023, 14(6): 454-461. |
| [5] | Fady Y. Hijji, Andrew D. Schneider, Matthew D. Thomas, Joseph G. Lyons, Daniel D. Bohl, Jennifer L. Jerele, Michael J. Prayson. Knowledge of radiation exposure associated with common trauma imaging modalities among orthopaedic surgeons, emergency medicine physicians, and general surgeons in the United States [J]. World Journal of Emergency Medicine, 2023, 14(4): 294-301. |
| [6] | Xinlei Wang, Yao Sun, Xiaoyu Ni, Shu Zhang. Development and validation of an emergency bloodstream infection score for predicting in-hospital mortality in patients with community-acquired bloodstream infections [J]. World Journal of Emergency Medicine, 2023, 14(4): 280-286. |
| [7] | Ahmed Faidh Ramzee, Ayman El-Menyar, Mohammad Asim, Ahad Kanbar, Khalid Ahmed, Bahaa Daoud, Saji Mathradikkal, Ahmad Kloub, Hassan Al-Thani, Sandro Rizoli. The impact of emergency department length of stay on the outcomes of trauma patients requiring hospitalization: a retrospective observational study [J]. World Journal of Emergency Medicine, 2023, 14(2): 96-105. |
| [8] | Jee Yen Kuck, Abdul Muhaimin Noor Azhar, Neena Wee, Rishya Manikam. Diagnostic accuracy of the tongue blade test combined with clinical signs to detect maxillary and mandibular fractures in the emergency department [J]. World Journal of Emergency Medicine, 2023, 14(2): 122-127. |
| [9] | Jing-jing Xu, Si-da Jia, Lin Jiang, Ying Song, Pei Zhu, De-shan Yuan, Yi Yao, Xue-yan Zhao, Jian-xin Li, Yue-jin Yang, Shu-bin Qiao, Bo Xu, Run-lin Gao, Jin-qing Yuan. Prolonged dual antiplatelet therapy after drug-eluting stent implantation improves long-term prognosis for acute coronary syndrome: five-year results from a large cohort study [J]. World Journal of Emergency Medicine, 2023, 14(1): 25-30. |
| [10] | Guang-mei Wang, Yong Li, Shuo Wu, Wen Zheng, Jing-jing Ma, Feng Xu, Jia-qi Zheng, He Zhang, Jia-li Wang, Yu-guo Chen. The combination of creatine kinase-myocardial band isoenzyme and point-of-care cardiac troponin/ contemporary cardiac troponin for the early diagnosis of acute myocardial infarction [J]. World Journal of Emergency Medicine, 2022, 13(3): 163-168. |
| [11] | Ittai Shichman, Or Shaked, Shai Factor, Ahuva Weiss-Meilik, Amal Khoury. Emergency department electric scooter injuries after the introduction of shared e-scooter services: A retrospective review of 3,331 cases [J]. World Journal of Emergency Medicine, 2022, 13(1): 5-10. |
| [12] | Ralphe Bou Chebl, Nader El Souki, Mirabelle Geha, Imad Majzoub, Rima Kaddoura, Hady Zgheib. Two-point compression ultrasonography: Enough to rule out lower extremity deep venous thrombosis? [J]. World Journal of Emergency Medicine, 2021, 12(4): 268-273. |
| [13] | Lori Stolz, Elaine Situ-LaCasse, Josie Acuña, Matthew Thompson, Nicolaus Hawbaker, Josephine Valenzuela, Uwe Stolz, Srikar Adhikari. What is the ideal approach for emergent pericardiocentesis using point-of-care ultrasound guidance? [J]. World Journal of Emergency Medicine, 2021, 12(3): 169-173. |
| [14] | Kun Cui, You-quan Shi, Yuan-zheng Zhang, Zheng-gong Li, Chang-ling Li. Optimized strategy of rotational atherectomy of underexpanded coronary stents in patients with acute coronary syndrome [J]. World Journal of Emergency Medicine, 2021, 12(3): 198-201. |
| [15] | Kasım Turgut, Erdal Yavuz, Mine Kayacı Yıldız, Mehmet Kaan Poyraz. Violence toward emergency physicians: A prospective-descriptive study [J]. World Journal of Emergency Medicine, 2021, 12(2): 111-116. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
