World Journal of Emergency Medicine ›› 2021, Vol. 12 ›› Issue (3): 169-173.doi: 10.5847/wjem.j.1920-8642.2021.03.001
• Original Articles • Next Articles
Lori Stolz1, Elaine Situ-LaCasse2, Josie Acuña2, Matthew Thompson3, Nicolaus Hawbaker4, Josephine Valenzuela5, Uwe Stolz1, Srikar Adhikari6( )
)
Received:2019-12-06
Accepted:2020-08-20
Online:2021-06-01
Published:2021-05-31
Contact:
Srikar Adhikari
E-mail:sriadhikari@aol.com
Lori Stolz, Elaine Situ-LaCasse, Josie Acuña, Matthew Thompson, Nicolaus Hawbaker, Josephine Valenzuela, Uwe Stolz, Srikar Adhikari. What is the ideal approach for emergent pericardiocentesis using point-of-care ultrasound guidance?[J]. World Journal of Emergency Medicine, 2021, 12(3): 169-173.
Add to citation manager EndNote|Ris|BibTeX
URL: http://wjem.com.cn/EN/10.5847/wjem.j.1920-8642.2021.03.001
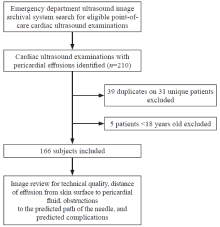
Figure 1.
Flow chart.
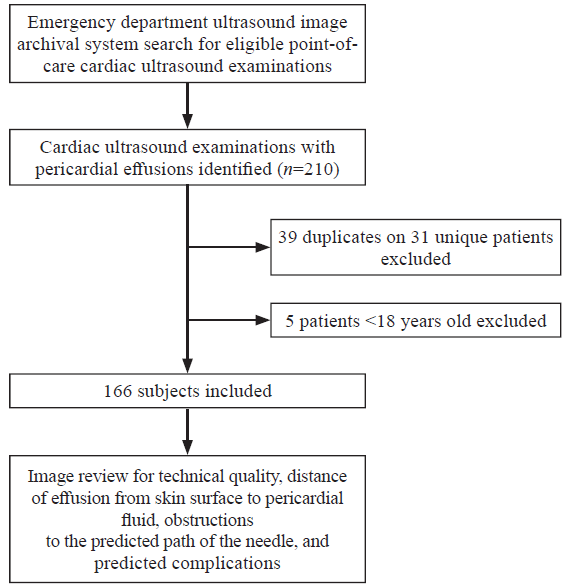
Table 1
Mean skin-to-pericardial fluid distance for each of the echocardiographic views
| Echocardiographic view | Mean skin-to-pericardial fluid distance, cm |
|---|---|
| Subxiphoid | 5.6 (95% CI 5.2-6.0) |
| Parasternal | 2.7 (95% CI 2.5-2.8) |
| Apical | 2.5 (95% CI 2.3-2.7) |
Table 2
Frequency of specific predicted complications for the subxiphoid view
| Predicted complication | Frequency | Percent |
|---|---|---|
| Liver in needle path | 82 | 49% |
| Prohibitive depth | 21 | 13% |
| Poor image quality | 20 | 12% |
| Movement (cardiac or respiratory) | 7 | 4% |
| Other | 8 | 5% |
| 1 |
Duvernoy O, Borowiec J, Helmius G, Erikson U. Complications of percutaneous pericardiocentesis under fluoroscopic guidance. Acta Radiol. 1992; 33(4):309-13.
pmid: 1633040 |
| 2 |
Bastian A, Meissner A, Lins M, Siegel EG, Möller F, Simon R. Pericardiocentesis: differential aspects of a common procedure. Intensive Care Med. 2000; 26(5):572-6.
doi: 10.1007/s001340051206 |
| 3 |
Tsang TS, Barnes ME, Hayes SN, Freeman WK, Dearani JA, Butler SL, et al. Clinical and echocardiographic characteristics of significant pericardial effusions following cardiothoracic surgery and outcomes of echo-guided pericardiocentesis for management: Mayo Clinic experience, 1979-1998. Chest. 1999; 116(2):322-31.
pmid: 10453858 |
| 4 |
Ho MY, Wang JL, Lin YS, Mao CT, Tsai ML, Wen MS, et al. Pericardiocentesis adverse event risk factors: a nationwide population-based cohort study. Cardiology. 2015; 130(1):37-45.
doi: 10.1159/000368796 |
| 5 |
Wong B, Murphy J, Chang CJ, Hassenein K, Dunn M. The risk of pericardiocentesis. Am J Cardiol. 1979; 44(6):1110-4.
pmid: 495505 |
| 6 | Bishop LH, Estes EJ, McIntosh JD. The electrocardiogram as a safeguard in pericardiocentesis. JAMA. 1956; 162(4):264-5. |
| 7 | Sinz E, Navarro K, Soderberg ES, Callaway CW. Advanced cardiovascular life support: provider manual. Dallas: American Heart Association; 2011: 1-142. |
| 8 | Committee on Trauma, American College of Surgeons. ATLS: advanced trauma life support for doctors (8th ed.). Chicago: American College of Surgeons; 2008: 129. |
| 9 | Harper RJ. Pericardiocentesis. In: Roberts JR, Hedges JR. Clinical Procedures in Emergency Medicine (5th ed.). Philadelphia: W.B Saunders; 2004: 211-5. |
| 10 | Buchman TG, Hall BL, Bowling WM, Kelen GD. Thoracic trauma. In: Tintinalli JE, Kelen GD, Stapczynski JS. Tintinalli’s emergency medicine: a comprehensive study guide (6th ed.). New York: McGraw-Hill; 2004: 1606-7. |
| 11 |
Tsang TS, Enriquez-Sarano M, Freeman WK, Barnes ME, Sinak LJ, Gersh BJ, et al. Consecutive 1127 therapeutic echocardiography-guided pericardiocentesis: clinical profile, practice patterns and outcomes spanning 21 years. Mayo Clin Proc. 2002; 77(5):429-36.
doi: 10.1016/S0025-6196(11)62211-8 |
| 12 |
Vayre F, Lardoux H, Pezzano M, Bourdarias JP, Dubourg O. Subxyphoid pericardiocentesis guided by contrast two-dimensional echocardiography in cardiac tamponade: experience of 110 consecutive patients. Eur J Echocardiogr. 2000; 1(1):66-71.
pmid: 12086218 |
| 13 |
No authors listed. Ultrasound guidelines: emergency, point-of-care and clinical ultrasound guidelines in medicine. Ann Emerg Med. 2017; 69(5):e27-54.
doi: 10.1016/j.annemergmed.2016.08.457 |
| 14 | American College of Emergency Physicians (ACEP) 2011; Emergency Ultrasound Standard Reporting Guidelines. Available at http://www.acep.org/workarea/DownloadAsset.aspx?id=82679. |
| 15 | Armstrong WF, Ryan T. Feigenbaum’s echocardiography (7th ed.). Philadelphia: Lippencott Williams and Wilkins; 2010: 242. |
| 16 |
Petri N, Ertel B, Gassenmaier T, Lengenfelder B, Bley TA, Voelker W. “Blind” pericardiocentesis: a comparison of different puncture directions. Catheter Cardiovasc Interv. 2018; 92(5):E327-32.
doi: 10.1002/ccd.v92.5 |
| 17 |
Osman A, Wan Chuan T, Ab Rahman J, Via G, Tavazzi G. Ultrasound-guided pericardiocentesis: a novel parasternal approach. Eur J Emerg Med. 2018; 25(5):322-7.
doi: 10.1097/MEJ.0000000000000471 pmid: 28509710 |
| 18 |
Hanaki Y, Kamiya H, Todoroki H, Yasui K, Ohsugi S, Ohno M, et al. New two dimensional ehocardiographically directed pericardiocentesis in cardiac tamponade. Crit Care Med. 1990; 18(7):750-3.
pmid: 2364716 |
| 19 |
Cho BC, Kang SM, Kim DH, Ko YG, Choi D, Ha JW, et al. Clinical and echocardiographic characteristics of pericardial effusion in patients who underwent echocardiographically guided pericardiocentesis: Yonsei Cardiovascular Center experience, 1993-2003. Yonsei Med J. 2004; 45(3):462-8.
doi: 10.3349/ymj.2004.45.3.462 |
| 20 |
Law MA, Borasino S, Kalra Y, Alten JA. Novel, long-axis in-plane ultrasound-guided pericardiocentesis for postoperative pericardial effusion drainage. Pediatr Cardiol. 2016; 37(7):1328-33.
doi: 10.1007/s00246-016-1438-z |
| 21 |
Sinnaeve PR, Adriaenssens T. A contemporary look at pericardiocentesis. Trends Cardiovasc Med. 2019; 29(7):375-83.
doi: 10.1016/j.tcm.2018.10.016 |
| [1] | Ralphe Bou Chebl, Nader El Souki, Mirabelle Geha, Imad Majzoub, Rima Kaddoura, Hady Zgheib. Two-point compression ultrasonography: Enough to rule out lower extremity deep venous thrombosis? [J]. World Journal of Emergency Medicine, 2021, 12(4): 268-273. |
| [2] | Kasım Turgut, Erdal Yavuz, Mine Kayacı Yıldız, Mehmet Kaan Poyraz. Violence toward emergency physicians: A prospective-descriptive study [J]. World Journal of Emergency Medicine, 2021, 12(2): 111-116. |
| [3] | Marin Pavlov, Lucija Klobučar, Iva Klobučar, Kristina Žgela, Vesna Degoricija. Does shifting to professional emergency department staffing affect the decision for chest radiography? [J]. World Journal of Emergency Medicine, 2021, 12(2): 87-92. |
| [4] | Hady Zgheib, Aline El Zakhem, Cynthia Wakil, Mohamad Ali Cheaito, Rola Cheaito, Antoine Finianos, Ralphe Bou Chebl, Rima Kaddoura, Nader Al Souky, Imad El Majzoub. Role of urine studies in asymptomatic febrile neutropenic patients presenting to the emergency department [J]. World Journal of Emergency Medicine, 2021, 12(2): 99-104. |
| [5] | William Gilliam, Jackson F. Barr, Brandon Bruns, Brandon Cave, Jordan Mitchell, Tina Nguyen, Jamie Palmer, Mark Rose, Safura Tanveer, Chris Yum, Quincy K. Tran. Factors associated with refractory pain in emergency patients admitted to emergency general surgery [J]. World Journal of Emergency Medicine, 2021, 12(1): 12-17. |
| [6] | Rebekah Shaw, Erica Popovsky, Alyssa Abo, Marni Jacobs, Nicole Herrera, James Chamberlain, Andrea Hahn. Improving antibiotic prescribing in the emergency department for uncomplicated community-acquired pneumonia [J]. World Journal of Emergency Medicine, 2020, 11(4): 199-205. |
| [7] | Hai-jiang Zhou, Tian-fei Lan, Shu-bin Guo. Outcome prediction value of National Early Warning Score in septic patients with community-acquired pneumonia in emergency department: A single-center retrospective cohort study [J]. World Journal of Emergency Medicine, 2020, 11(4): 206-215. |
| [8] | Chuan-qi Ding, Yu-ping Zhang, Yu-wei Wang, Min-fei Yang, Sa Wang, Nian-qi Cui, Jing-fen Jin. Death and do-not-resuscitate order in the emergency department: A single-center three-year retrospective study in the Chinese mainland [J]. World Journal of Emergency Medicine, 2020, 11(4): 231-237. |
| [9] | Maybritt I. Kuypers, Adinda Klijn, Nieke E. Mullaart-Jansen, Frans B. Plötz. Availability and quality of procedural sedation and analgesia in emergency departments without emergency physicians: A national survey in the Netherlands [J]. World Journal of Emergency Medicine, 2020, 11(2): 69-73. |
| [10] | Emily Shao, Chantelle Judge, Erin McMeniman, Tina Bazianas, Rob Eley. Presenting patterns of dermatology conditions to an Australian emergency department [J]. World Journal of Emergency Medicine, 2020, 11(2): 74-78. |
| [11] | Zhenghong Liu, Mingwei Ng, Dinesh V. Gunasekeran, Huihua Li, Kishanti Ponampalam, R Ponampalam. Mobile technology: Usage and perspective of patients and caregivers presenting to a tertiary care emergency department [J]. World Journal of Emergency Medicine, 2020, 11(1): 5-11. |
| [12] | Samantha Shwe, Lauren Witchey, Shadi Lahham, Ethan Kunstadt, Inna Shniter, John C. Fox. Retrospective analysis of eFAST ultrasounds performed on trauma activations at an academic level-1 trauma center [J]. World Journal of Emergency Medicine, 2020, 11(1): 12-17. |
| [13] | Elaine Situ-LaCasse, Helpees Guirguis, Lucas Friedman, Asad E. Patanwala, Seth E. Cohen, Srikar Adhikari. Can emergency physicians perform extended compression ultrasound for the diagnosis of lower extremity deep vein thrombosis? [J]. World Journal of Emergency Medicine, 2019, 10(4): 205-209. |
| [14] | Wirachin Hoonpongsimanont, Preet Kaur Sahota, Yanjun Chen, Maria Nguyen, Christine Louis, Jonathan Pena, Andrew Wong, Maxwell Jen. Emergency department patient experience: Same location, same provider, different scores by different survey methods [J]. World Journal of Emergency Medicine, 2019, 10(3): 138-144. |
| [15] | Chang Pan, Xiao-ran Huang, Jiao-jiao Pang, Kai Cheng, Feng Xu, Yu-guo Chen. Trends in mortality of emergency departments patients in China [J]. World Journal of Emergency Medicine, 2019, 10(3): 152-155. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
