World Journal of Emergency Medicine ›› 2021, Vol. 12 ›› Issue (1): 12-17.doi: 10.5847/wjem.j.1920-8642.2021.01.002
• Original Articles • Previous Articles Next Articles
William Gilliam1, Jackson F. Barr2, Brandon Bruns3,4, Brandon Cave2, Jordan Mitchell2, Tina Nguyen5, Jamie Palmer6, Mark Rose2, Safura Tanveer2, Chris Yum2, Quincy K. Tran3,7( )
)
Received:2019-12-25
Accepted:2020-06-26
Online:2021-01-01
Published:2021-01-01
Contact:
Quincy K. Tran
E-mail:qtran@som.umaryland.edu
William Gilliam, Jackson F. Barr, Brandon Bruns, Brandon Cave, Jordan Mitchell, Tina Nguyen, Jamie Palmer, Mark Rose, Safura Tanveer, Chris Yum, Quincy K. Tran. Factors associated with refractory pain in emergency patients admitted to emergency general surgery[J]. World Journal of Emergency Medicine, 2021, 12(1): 12-17.
Add to citation manager EndNote|Ris|BibTeX
URL: http://wjem.com.cn/EN/10.5847/wjem.j.1920-8642.2021.01.002
Figure 1.
Patient selection diagram. ED: emergency department; EGS: emergency general surgery; NRS: numerating rate scale.
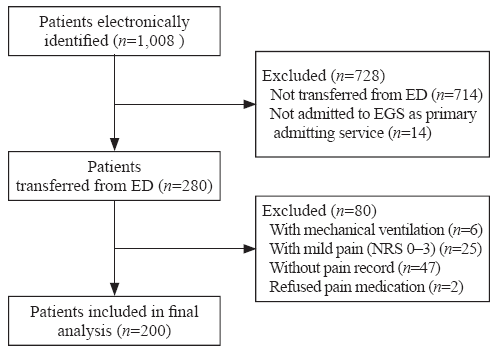
Table 1
Characteristics of ED patients who were admitted to EGS for evaluation and management
| Parameters | All patients |
|---|---|
| Total patients, n (%) | 200 (100) |
| Gender, n (%) | |
| Male | 88 (44) |
| Female | 112 (56) |
| Age in years, mean±SD | 55±19 |
| Past medical history, n (%) | |
| CHF | 13 (7) |
| Hypertension | 95 (48) |
| DM | 36 (18) |
| Any liver disease | 13 (7) |
| Any kidney disease | 12 (6) |
| ESI, median (IQR) | 3 (2-3) |
| Triage systolic blood pressure (mmHg), mean±SD | 133±20 |
| Triage heart rate (bpm), mean±SD | 94±19 |
| Triage pain score, mean±SD | 8±2 |
| Triage GCS, median (IQR) | 15 (14-15) |
| ED LOS (minutes), median (IQR) | 491 ( 327-728) |
| Pain score at departure, mean±SD | 5±3 |
| Total MEU, mean±SD | 12±11 |
| Total IVF (liter), mean±SD | 1.4±1.0 |
| Refractory pain at ED departure, n (%) | 58 (29) |
| ED diagnosis, n (%) | |
| Appendicitis | 4 (2) |
| Bowel obstruction | 40 (20) |
| Bowel perforation | 30 (15) |
| Bowel ischemia | 16 (8) |
| GI bleeding | 12 (6) |
| Hernia | 13 (7) |
| Intra-abdominal infection | 28 (14) |
| Pancreatitis | 18 (9) |
| Other | 39 (20) |
| Operation, n (%) | |
| None | 70 (35) |
| Laparotomy | 61 (31) |
| Laparoscopy | 26 (13) |
| Endoscopy | 10 (5) |
| Percutaneous intervention by IR | 9 (4) |
| Incision and drainage | 9 (4) |
| Other | 15 (8) |
| Mortality, n (%) | 8 (4) |
| Hospital length of stay (days), median (IQR) | 6 (3-10) |
Table 2
Comparison of clinical factors between patients with and without refractory pain
| Parameters | All (n=200) | No refractory pain (group A) (n=142) | Refractory pain (group B) (n=58) | P-value (A vs. B) |
|---|---|---|---|---|
| SOFA score, mean±SD | 2±1 | 2±1 | 3±2 | 0.001 |
| Shock index, mean±SD | 0.86±0.30 | 0.80±0.30 | 0.95±0.40 | 0.030 |
| WBC (×109/L), mean±SD | 13±7 | 13±7 | 15±8 | 0.034 |
| Lactate (mg/dL), mean±SD | 1.9±1.8 | 1.4±0.9 | 3.4±2.0 | 0.001 |
| Triage GCS, median (IQR) | 15 (14-15) | 15 (14-15) | 15 (14-15) | 0.510 |
| Triage pain score, mean±SD | 8±2 | 8±2 | 8±1 | 0.400 |
| Triage SBP (mmHg), mean±SD | 133±20 | 135±27 | 127±32 | 0.070 |
| Triage heart rate (beats per minute), mean±SD | 94±19 | 93±18 | 97±23 | 0.220 |
| Pain score at ED departure, mean±SD | 5±3 | 4±3 | 8±2 | 0.001 |
| Change of pain score, mean±SD | -3±3 | -5±2 | 0±1 | 0.001 |
| ED length of stay (minutes), median (IQR) | 491 (327-728) | 524 (359-774) | 355 (233-570) | 0.001 |
| Mortality, n (%) | 8 (4) | 3 (2) | 5 (9) | 0.047 |
| Hospital length of stay (days), median (IQR) | 6 (3-10) | 6 (3-9) | 9 (4-15) | 0.002 |
Table 3
Comparison of ED interventions for patients with and without refractory pain
| Parameters | All (n=200) | No refractory pain (group A) (n=142) | Refractory pain (group B) (n=58) | P-value (A vs. B) |
|---|---|---|---|---|
| Number of pain medication administration, median (IQR) | 4 (3-6) | 4 (3-7) | 3 (3-5) | 0.001 |
| Pain medication type, n (%)* | ||||
| No pain medication | 26 (13) | 13 (9) | 13 (22) | 0.020 |
| Any opioids | 164 (82) | 123 (87) | 41 (70) | 0.010 |
| Opioids+non-opioids | 20 (10) | 14 (10) | 6 (10) | 0.890 |
| Non-opioids | 30 (15) | 20 (14) | 10 (17) | 0.730 |
| Total MEU, mean±SD | 22±11 | 13±9 | 9±16 | 0.020 |
| MEU per kg (body weight), mean±SD | 0.15±0.16 | 0.18±0.20 | 0.11±0.10 | 0.004 |
| Total intravenous crystalloids (liter), mean±SD | 1.4±1.0 | 1.2±0.9 | 1.8±1.2 | 0.017 |
| IVF per kg, mean±SD | 17±1 | 16±14 | 21±17 | 0.060 |
| Any anti-emetics, n (%) | 134 (67) | 97 (68) | 37 (64) | 0.650 |
| Total number of antibiotics, median (IQR) | 0 (0-1) | 0 (0-1) | 1 (0-2) | 0.038 |
| Receiving any antibiotics, n (%) | 92 (46) | 60 (42) | 32 (55) | 0.130 |
Table 4
Results from multivariable logistic regression to assess clinical factors and refractory pain among patients admitted to emergency general surgery from emergency departments
| Independent variables | Univariate logistic regression | Multivariable logistic regression | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | P-value | OR | 95% CI | P-value | |
| Serum lactate | 4.60 | 2.80-7.60 | 0.001 | 3.80 | 2.10-6.80 | 0.001 |
| Number of pain medication administration | 0.84 | 0.75-0.95 | 0.001 | 0.80 | 0.68-0.98 | 0.020 |
| Gender - male | 2.30 | 1.20-4.40 | 0.008 | 1.80 | 0.65-5.20 | 0.250 |
| Past medical history - any kidney disease | 2.30 | 1.20-4.30 | 0.080 | 1.90 | 0.40-9.10 | 0.430 |
| Emergency Severity Index | 0.55 | 0.30-0.97 | 0.040 | 0.60 | 0.20-1.90 | 0.420 |
| SOFA | 1.40 | 1.20-1.70 | 0.001 | 1.10 | 0.80-1.50 | 0.570 |
| Triage SBP | 0.98 | 0.98-1.00 | 0.047 | 1.01 | 0.98-1.03 | 0.350 |
| WBC | 1.04 | 1.00-1.08 | 0.033 | 0.90 | 0.90-1.04 | 0.350 |
| MEU per kg (body weight)* | 0.05 | 0.00-0.60 | 0.007 | 0.10 | 0.01-1.50 | 0.380 |
| Opioids+non-opioids* | 1.30 | 0.50-3.70 | 0.590 | 1.60 | 0.40-6.30 | 0.490 |
| IVF per kg (body weight)* | 1.02 | 1.01-1.04 | 0.044 | 0.98 | 0.90-1.02 | 0.460 |
| Number of antibiotics | 1.50 | 1.03-2.10 | 0.032 | 1.60 | 0.90-2.80 | 0.090 |
| Diagnosis - bowel obstruction | 0.40 | 0.10-0.90 | 0.022 | 0.80 | 0.20-2.80 | 0.690 |
| Diagnosis - bowel perforation | 2.10 | 0.90-5.00 | 0.087 | 0.60 | 0.10-2.90 | 0.530 |
| 1 |
Rupp T, Delaney KA. Inadequate analgesia in emergency medicine. Ann Emerg Med. 2004; 43(4):494-503.
pmid: 15039693 |
| 2 |
Todd KH, Ducharme J, Choiniere M, Crandall CS, Fosnocht DE, Homel P, et al. Pain in the emergency department: results of the pain and emergency medicine initiative (PEMI) multicenter study. J Pain. 2007; 8(6):460-6.
doi: 10.1016/j.jpain.2006.12.005 pmid: 17306626 |
| 3 |
Connor AB, Zwemer FL, Hays DP, Feng C. Outcomes after intravenous opioids in emergency patients: a prospective cohort analysis. Acad Emerg Med. 2009; 16(6):477-87.
doi: 10.1111/j.1553-2712.2009.00405.x pmid: 19426295 |
| 4 |
Vila H Jr, Smith RA, Augustyniak MJ, Nagi PA, Soto RG, Ross TW, et al. The efficacy and safety of pain management before and after implementation of hospital-wide pain management standards: is patient safety compromised by treatment based solely on numerical pain ratings? Anesth Analg. 2005; 101(2):474-80.
doi: 10.1213/01.ANE.0000155970.45321.A8 pmid: 16037164 |
| 5 |
Muntlin Å, Gunningberg L, Carlsson M. Patients’ perceptions of quality of care at an emergency department and identification of areas for quality improvement. J Clin Nurs. 2006; 15(8):1045-56.
pmid: 16879549 |
| 6 |
Raso R. Value-based purchasing: what’s the score? Reward or penalty, step up to the plate. Nurs Manage. 2013; 44(5):28-34.
pmid: 23571763 |
| 7 |
Miner J, Biros MH, Trainor A, Hubbard D, Beltram M. Patient and physician perceptions as risk factors for oligoanalgesia: a prospective observational study of the relief of pain in the emergency department. Acad Emerg Med. 2006; 13(2):140-6.
doi: 10.1197/j.aem.2005.08.008 pmid: 16436793 |
| 8 |
Tran QK, Nguyen T, Tuteja G, Tiffany L, Aitken A, Jones K, et al. Emergency providers’ pain management in patients transferred to intensive care unit for urgent surgical interventions. West J Emerg Med. 2018; 19(5):877-83.
pmid: 30202502 |
| 9 |
Tran QK, O’Connor J, Vesselinov R, Haase D, Duncan R, Aitken A, et al. The critical care resuscitation unit transfers more patients from emergency departments faster and is associated with improved outcomes. J Emerg Med. 2020; 58(2):280-9.
doi: 10.1016/j.jemermed.2019.09.041 pmid: 31761462 |
| 10 |
Bruns BR, Tesoriero R, Narayan M, Klyushnenkova EN, Chen H, Scalea TM, et al. Emergency general surgery: defining burden of disease in the State of Maryland. Am Surg. 2015; 81(8):829-34.
pmid: 26215249 |
| 11 | Cepeda MS, Africano JM, Polo R, Alcala R, Carr DB. What decline in pain intensity is meaningful to patients with acute pain? Pain. 2003; 105(1/2):151-7. |
| 12 |
Jao K, McD Taylor D, Taylor SE, Khan M, Chae J. Simple clinical targets associated with a high level of patient satisfaction with their pain management. Emerg Med Australas. 2011; 23(2):195-201.
pmid: 21489167 |
| 13 |
Yelverton S, Rozario N, Matthews BD, Reinke CE. Interhospital transfer for emergency general surgery: an independent predictor of mortality. Am J Surg. 2018; 216(4):787-92.
doi: 10.1016/j.amjsurg.2018.07.055 pmid: 30166049 |
| 14 |
Patanwala AE, Duby J, Waters D, Erstad BL. Opioid conversions in acute care. Ann Pharmacother. 2007; 41(2):255-67.
doi: 10.1345/aph.1H421 |
| 15 | Wolfe J, Lein D, Lenkoski K, Smithline H. Analgesic administration to patients with an acute abdomen: a survey of emergency medicine physicians. Am J Emerg Med. 2000; 28(3):250-3. |
| 16 | Garcia-Alvarez M, Marik P, Bellomo R. Sepsis-associated hyperlactatemia. Crit Care. 2014; 18(5):1-11. |
| 17 |
Wang YY, Chang RB, Allgood SD, Silver WL, Liman ER. A TRPA1-dependent mechanism for the pungent sensation of weak acids. J Gen Physiol. 2011; 137(6):493-505.
doi: 10.1085/jgp.201110615 pmid: 21576376 |
| 18 |
Wang X, Li WG, Yu Y, Xiao X, Cheng J, Zeng WZ, et al. Serotonin facilitates peripheral pain sensitivity in a manner that depends on the nonproton ligand sensing domain of ASIC3 channel. J Neurosci. 2013; 33(10):4265-79.
pmid: 23467344 |
| 19 |
Kim TJ, Freml L, Park SS, Brennan TJ. Lactate concentrations in incisions indicate ischemic-like conditions may contribute to postoperative pain. J Pain. 2007; 8(1):59-66.
pmid: 16949881 |
| 20 |
Bijur PE, Kenny MK, Gallagher EJ. Intravenous morphine at 0.1 mg/kg is not effective for controlling severe acute pain in the majority of patients. Ann Emerg Med. 2005; 46(4):362-7.
doi: 10.1016/j.annemergmed.2005.03.010 pmid: 16187470 |
| [1] | Ralphe Bou Chebl, Nader El Souki, Mirabelle Geha, Imad Majzoub, Rima Kaddoura, Hady Zgheib. Two-point compression ultrasonography: Enough to rule out lower extremity deep venous thrombosis? [J]. World Journal of Emergency Medicine, 2021, 12(4): 268-273. |
| [2] | Lori Stolz, Elaine Situ-LaCasse, Josie Acuña, Matthew Thompson, Nicolaus Hawbaker, Josephine Valenzuela, Uwe Stolz, Srikar Adhikari. What is the ideal approach for emergent pericardiocentesis using point-of-care ultrasound guidance? [J]. World Journal of Emergency Medicine, 2021, 12(3): 169-173. |
| [3] | Kasım Turgut, Erdal Yavuz, Mine Kayacı Yıldız, Mehmet Kaan Poyraz. Violence toward emergency physicians: A prospective-descriptive study [J]. World Journal of Emergency Medicine, 2021, 12(2): 111-116. |
| [4] | Marin Pavlov, Lucija Klobučar, Iva Klobučar, Kristina Žgela, Vesna Degoricija. Does shifting to professional emergency department staffing affect the decision for chest radiography? [J]. World Journal of Emergency Medicine, 2021, 12(2): 87-92. |
| [5] | Hady Zgheib, Aline El Zakhem, Cynthia Wakil, Mohamad Ali Cheaito, Rola Cheaito, Antoine Finianos, Ralphe Bou Chebl, Rima Kaddoura, Nader Al Souky, Imad El Majzoub. Role of urine studies in asymptomatic febrile neutropenic patients presenting to the emergency department [J]. World Journal of Emergency Medicine, 2021, 12(2): 99-104. |
| [6] | Rebekah Shaw, Erica Popovsky, Alyssa Abo, Marni Jacobs, Nicole Herrera, James Chamberlain, Andrea Hahn. Improving antibiotic prescribing in the emergency department for uncomplicated community-acquired pneumonia [J]. World Journal of Emergency Medicine, 2020, 11(4): 199-205. |
| [7] | Hai-jiang Zhou, Tian-fei Lan, Shu-bin Guo. Outcome prediction value of National Early Warning Score in septic patients with community-acquired pneumonia in emergency department: A single-center retrospective cohort study [J]. World Journal of Emergency Medicine, 2020, 11(4): 206-215. |
| [8] | Chuan-qi Ding, Yu-ping Zhang, Yu-wei Wang, Min-fei Yang, Sa Wang, Nian-qi Cui, Jing-fen Jin. Death and do-not-resuscitate order in the emergency department: A single-center three-year retrospective study in the Chinese mainland [J]. World Journal of Emergency Medicine, 2020, 11(4): 231-237. |
| [9] | Maybritt I. Kuypers, Adinda Klijn, Nieke E. Mullaart-Jansen, Frans B. Plötz. Availability and quality of procedural sedation and analgesia in emergency departments without emergency physicians: A national survey in the Netherlands [J]. World Journal of Emergency Medicine, 2020, 11(2): 69-73. |
| [10] | Emily Shao, Chantelle Judge, Erin McMeniman, Tina Bazianas, Rob Eley. Presenting patterns of dermatology conditions to an Australian emergency department [J]. World Journal of Emergency Medicine, 2020, 11(2): 74-78. |
| [11] | Zhenghong Liu, Mingwei Ng, Dinesh V. Gunasekeran, Huihua Li, Kishanti Ponampalam, R Ponampalam. Mobile technology: Usage and perspective of patients and caregivers presenting to a tertiary care emergency department [J]. World Journal of Emergency Medicine, 2020, 11(1): 5-11. |
| [12] | Wirachin Hoonpongsimanont, Preet Kaur Sahota, Yanjun Chen, Maria Nguyen, Christine Louis, Jonathan Pena, Andrew Wong, Maxwell Jen. Emergency department patient experience: Same location, same provider, different scores by different survey methods [J]. World Journal of Emergency Medicine, 2019, 10(3): 138-144. |
| [13] | Chang Pan, Xiao-ran Huang, Jiao-jiao Pang, Kai Cheng, Feng Xu, Yu-guo Chen. Trends in mortality of emergency departments patients in China [J]. World Journal of Emergency Medicine, 2019, 10(3): 152-155. |
| [14] | Rakesh Gupta, Isaac Siemens, Sam Campbell. The use of outcome feedback by emergency medicine physicians: Results of a physician survey [J]. World Journal of Emergency Medicine, 2019, 10(1): 14-18. |
| [15] | Elaine Situ-LaCasse, Ryan W. Grieger, Stephen Crabbe, Anna L. Waterbrook, Lucas Friedman, Srikar Adhikari. Utility of point-of-care musculoskeletal ultrasound in the evaluation of emergency department musculoskeletal pathology [J]. World Journal of Emergency Medicine, 2018, 9(4): 262-266. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
