World Journal of Emergency Medicine ›› 2022, Vol. 13 ›› Issue (6): 453-458.doi: 10.5847/wjem.j.1920-8642.2022.103
• Original Articles • Previous Articles Next Articles
Gui-ying Dong1, Fei-fei Jin2, Qi Huang3, Chun-bo Wu1, Ji-hong Zhu1( ), Tian-bing Wang2()
), Tian-bing Wang2()
Received:2022-03-09
Accepted:2022-06-10
Online:2022-09-16
Published:2022-11-01
Contact:
Ji-hong Zhu,Tian-bing Wang
E-mail:zhujihong642021@163.com;wangtianbing@pkuph.edu.cn
Gui-ying Dong, Fei-fei Jin, Qi Huang, Chun-bo Wu, Ji-hong Zhu, Tian-bing Wang. Exploratory COVID-19 death risk score based on basic laboratory tests and physiological clinical measurements[J]. World Journal of Emergency Medicine, 2022, 13(6): 453-458.
Add to citation manager EndNote|Ris|BibTeX
URL: http://wjem.com.cn/EN/10.5847/wjem.j.1920-8642.2022.103

Figure 1.
The flow chart of this study.
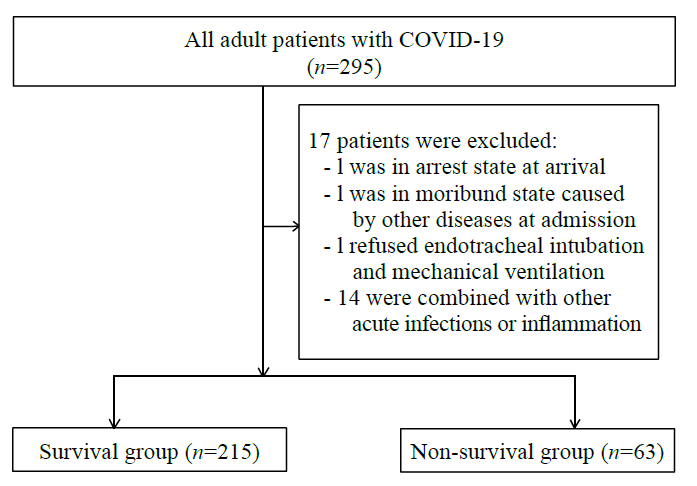
Table 1.
Baseline demographics and clinical characteristics
| Variables | All (n=278) | Survival (n=215) | Non-survival (n=63) | P-value |
|---|---|---|---|---|
| Demographics | ||||
| Male | 146 (52.52) | 107 (49.77) | 39 (61.90) | 0.090 |
| Age, years | 64 (52-71) | 61 (49-69) | 70 (62-80) | <0.001* |
| Youth (18-65 years) | 156 (56.12) | 136 (63.26) | 20 (31.75) | <0.001* |
| Middle-aged (66-79 years) | 92 (33.09) | 66 (30.70) | 26 (41.27) | 0.185 |
| Elderly (80-99 years) | 30 (10.79) | 13 (6.05) | 17 (26.98) | <0.001* |
| Comorbidity | ||||
| Hypertension | 113 (40.65) | 86 (40.00) | 27 (42.86) | 0.685 |
| Diabetes mellitus | 57 (20.50) | 39 (18.14) | 18 (28.57) | 0.071 |
| Cardiovascular disease | 53 (19.06) | 34 (15.81) | 19 (30.16) | 0.011* |
| Chronic pulmonary disease | 25 (8.99) | 14 (6.51) | 11 (17.46) | 0.008* |
| Chronic kidney disease | 16 (5.76) | 15 (6.98) | 1 (1.59) | 0.102 |
| Malignancy tumor | 10 (3.60) | 6 (2.79) | 4 (6.35) | 0.182 |
| Chronic liver disease | 7 (2.52) | 4 (1.86) | 5 (7.94) | 0.017* |
| Intervention during hospital | ||||
| Mechanical ventilation | 71 (25.54) | 11 (5.11) | 60 (95.24) | <0.001* |
| Vasoactive drug therapy | 42 (15.11) | 4 (1.86) | 42 (66.67) | <0.001* |
Table 2.
Univariate and multivariate regression analysis of the risk factors for 30-day mortality
| Risk factors | Univariate regression analysis | Multivariate regression analysis | |||
|---|---|---|---|---|---|
| OR (95%CI) | P-value | OR (95%CI) | P-value | ||
| Age | 1.066 (1.040-1.094) | <0.001* | 1.080 (0.979-1.193) | 0.126 | |
| RR | 1.292 (1.212-1.376) | <0.001* | 1.185 (1.032-1.361 ) | 0.016* | |
| WBC | 1.505 (1.351-1.678) | <0.001* | 1.131 (0.943-1.358) | 0.185 | |
| D-dimer | 1.264 (1.199-1.334) | <0.001* | 1.101 (0.986-1.229) | 0.089* | |
| hsCRP | 1.026 (1.020-1.033) | <0.001* | 1.018 (1.003-1.033) | 0.017* | |
| IL-6 | 1.024 (1.017-1.031) | <0.001* | 1.003 (0.992-1.014) | 0.628 | |
| Ferritin | 1.001 (1.001-1.002) | <0.001* | 1.001 (1.000-1.002) | 0.207 | |
| hsTnI | 1.002 (1.001-1.003) | 0.001* | 1.000 (1.000-1.000) | 0.606 | |
| NT-proBNP | 1.000 (1.000-1.000) | <0.001* | 1.000 (1.000-1.000) | 0.272 | |
| Scr | 1.003 (1.002-1.005) | <0.001* | 1.002 (0.999-1.006) | 0.192 | |
| ALT | 1.013 (1.006-1.019) | <0.001* | 1.015 (0.987-1.042) | 0.298 | |
Table 3.
The performance comparison of CDRS with SOFA and CURB-65
| Scores | All (n=278) | Survival (n=215) | Non-survival (n=63) | P-value | AUC (95% CI) | Cut-off |
|---|---|---|---|---|---|---|
| CDRS | -2.80 (-5.72 - -1.01) | -4.71 (-6.05 - -3.96) | 3.71 (1.12-6.54) | <0.001* | 0.984 (0.969-0.998) | -1.14 |
| SOFA | 2 (0-4) | 1 (0-2) | 12 (8-15) | <0.001* | 0.975 (0.945-1.000) | 5 |
| CURB-65 | 1 (0-2) | 1 (0-1) | 4 (3-5) | <0.001* | 0.971 (0.949-0.994) | 3 |

Figure 2.
Calibration curves constructed using the bootstrap (n=278). CDRS: COVID-19 death risk score.
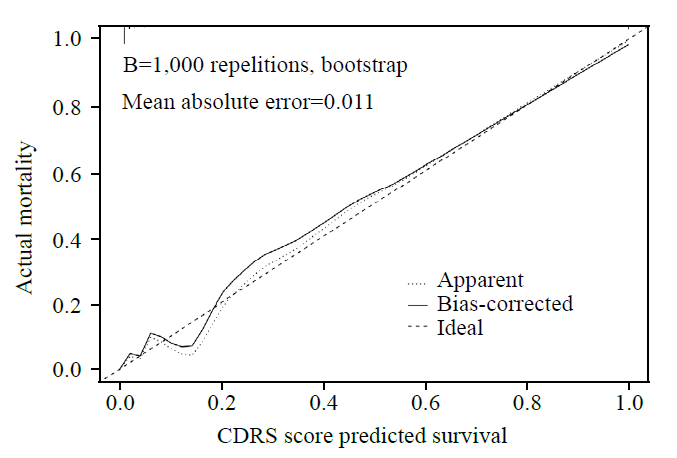

Figure 3.
The decision curve analysis (DCA) curves of medical intervention in patients with the CDRS, SOFA, and CURB-65. CDRS: COVID-19 death risk score; SOFA: sequential organ failure assessment; CURB-65: confusion, uremia, respiratory rate, blood pressure and age ≥ 65 years.

| 1 | Du B, Wang CT, Singer M. Learning for the next pandemic: the Wuhan experience of managing critically ill people. BMJ. 2021; 375:e066090. |
| 2 | National Health Commission of the People’s Republic of China. Guideline for the diagnosis and treatment of COVID-19 infections (version1-7). 2020. Available at: http://www.nhc.gov.cn/yzygj/zcwj2/new_zcwj.shtml |
| 3 |
Smilowitz NR, Nguy V, Aphinyanaphongs Y, Newman JD, Xia YH, Reynolds HR, et al. Multiple biomarker approach to risk stratification in COVID-19. Circulation. 2021; 143(13): 1338-40.
doi: 10.1161/CIRCULATIONAHA.120.053311 |
| 4 |
Zakeri R, Pickles A, Carr E, Bean DM, O’Gallagher K, Kraljewic Z, et al. Biological responses to COVID-19: insights from physiological and blood biomarker profiles. Curr Res Transl Med. 2021; 69(2):103276.
doi: 10.1016/j.retram.2021.103276 |
| 5 |
Oldoni E, van Gool A, García Bermejo L, Scherer A, Mayrhofer MT, Florindi F, et al. Biomarker research and development for coronavirus disease 2019 (COVID-19): European medical research infrastructures call for global coordination. Clin Infect Dis. 2021; 72(10):1838-42.
doi: 10.1093/cid/ciaa1250 pmid: 33091118 |
| 6 |
Bivona G, Agnello L, Ciaccio M. Biomarkers for prognosis and treatment response in COVID-19 patients. Ann Lab Med. 2021; 41(6):540-8.
doi: 10.3343/alm.2021.41.6.540 pmid: 34108281 |
| 7 | Kamran F, Tang SP, Otles E, McEvoy DS, Saleh SN, Gong J, et al. Early identification of patients admitted to hospital for covid-19 at risk of clinical deterioration: model development and multisite external validation study. BMJ. 2022; 376:e068576. |
| 8 |
Gupta RK, Harrison EM, Ho A, Docherty AB, Knight SR, van Smeden M, et al. Development and validation of the ISARIC 4C deterioration model for adults hospitalised with COVID-19: a prospective cohort study. Lancet Respir Med. 2021; 9(4):349-59.
doi: 10.1016/S2213-2600(20)30559-2 pmid: 33444539 |
| 9 | Berenguer J, Borobia AM, Ryan P, Rodríguez-Baño J, Bellón JM, Jarrín I, et al. Development and validation of a prediction model for 30-day mortality in hospitalised patients with COVID-19: the COVID-19 SEIMC score. Thorax. 2021;76(9): 920-9. |
| 10 |
Heber S, Pereyra D, Schrottmaier WC, Kammerer K, Santol J, Rumpf B, et al. A model predicting mortality of hospitalized covid-19 patients four days after admission: development, internal and temporal-external validation. Front Cell Infect Microbiol. 2022; 11:795026.
doi: 10.3389/fcimb.2021.795026 |
| 11 |
Bellou V, Tzoulaki I, van Smeden M, Moons KGM, Evangelou E, Belbasis L. Prognostic factors for adverse outcomes in patients with COVID-19: a field-wide systematic review and meta-analysis. Eur Respir J. 2022; 59(2):2002964.
doi: 10.1183/13993003.02964-2020 |
| 12 |
Signorini SG, Brugnoni D, Levaggi R, Garrafa E. Less is more: an ecological and economic point of view on appropriate use of lab testing for COVID-19 patients. Bioanalysis. 2021; 13(24):1781-3.
doi: 10.4155/bio-2021-0064 pmid: 34355575 |
| 13 |
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007; 335(7624):806-8.
doi: 10.1136/bmj.39335.541782.AD |
| 14 |
Vincent JL, Moreno R, Takala J, Willatts S, Bruining H, et al. The SOFA (sepsis-related organ failure assessment) score to describe organ dysfunction/failure. On behalf of the working group on sepsis-related problems of the European society of intensive care medicine. Intensive Care Med. 1996; 22(7):707-10.
doi: 10.1007/BF01709751 |
| 15 | Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007 ;44(Suppl 2):S27-S72. |
| 16 |
Mayer TA, Walker ML. Pediatric head injury: the critical role of the emergency physician. Ann Emerg Med. 1985; 14(12):1178-84.
pmid: 4061990 |
| 17 | Chen W, Janz DR, Shaver CM, Bernard GR, Bastarache JA, Ware LB. Clinical characteristics and outcomes are similar in ARDS diagnosed by oxygen saturation//FiO2 ratio compared with PaO2/FiO2 ratio. Chest. 2015; 48(6):1477-83. |
| 18 |
Dong GY, Du Z, Zhu JH, Guo Y, Gao WB, Guo W, et al. The clinical characteristics and prognosis of COVID-19 patients with comorbidities: a retrospective analysis of the infection peak in Wuhan. Ann Transl Med. 2021; 9(4):280.
doi: 10.21037/atm-20-4052 pmid: 33708907 |
| 19 |
Collins GS, Reitsma JB, Altman DG, Moons KG. Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD): the TRIPOD statement. Ann Intern Med. 2015; 162(1):55-63.
doi: 10.7326/M14-0697 pmid: 25560714 |
| 20 |
Shi L, Wang Y, Wang YD, Duan GC, Yang HY. Dyspnea rather than fever is a risk factor for predicting mortality in patients with COVID-19. J Infect. 2020; 81(4):647-79.
doi: S0163-4453(20)30288-7 pmid: 32417316 |
| 21 |
Ko JY, Danielson ML, Town M, Derado G, Greenlund KJ, Kirley PD, et al. Risk factors for coronavirus disease 2019 (COVID-19)-associated hospitalization: COVID-19-associated hospitalization surveillance network and behavioral risk factor surveillance system. Clin Infect Dis. 2021; 72(11):e695-e703.
doi: 10.1093/cid/ciaa1419 pmid: 32945846 |
| 22 | Rothman KJ. Epidemiology:an Introduction. New York: Oxford University Press. 2002. |
| 23 |
Raschke RA, Agarwal S, Rangan P, Heise CW, Curry SC. Discriminant accuracy of the SOFA score for determining the probable mortality of patients with COVID-19 pneumonia requiring mechanical ventilation. JAMA. 2021; 325(14):1469-70.
doi: 10.1001/jama.2021.1545 pmid: 33595630 |
| 24 |
Elmoheen A, Abdelhafez I, Salem W, Bahgat M, Elkandow A, Tarig A, et al. External validation and recalibration of the CURB-65 and PSI for predicting 30-day mortality and critical care intervention in multiethnic patients with COVID-19. Int J Infect Dis. 2021; 111:108-16.
doi: 10.1016/j.ijid.2021.08.027 pmid: 34416403 |
| 25 | World Health Organization. Ageing: preventing and managing the global epidemic:report on a WHO consultation. Geneva: World Health Organization; 2000. (WHO Technical Report Series 894). |
| 26 | Hong Kong Health Organization. Coronavirus disease (COVID-2019) situation report. Available at: https://www.chp.gov.hk/en/index.html |
| 27 |
Karim S, Karim QA. Omicron SARS-CoV-2 variant: a new chapter in the COVID-19 pandemic. Lancet. 2021; 398(10317): 2126-8.
doi: 10.1016/S0140-6736(21)02758-6 pmid: 34871545 |
| 28 |
Martínez-Lacalzada M, Viteri-Noël A, Manzano L, Fabregate M, Rubio-Rivas M, Luis García S, et al. Predicting critical illness on initial diagnosis of COVID-19 based on easily obtained clinical variables: development and validation of the PRIORITY model. Clin Microbiol Infect. 2021; 27(12):1838-44.
doi: 10.1016/j.cmi.2021.07.006 |
| 29 | Soltan AAS, Kouchaki S, Zhu TT, Kiyasseh D, Taylor T, Hussain ZB, et al. Rapid triage for COVID-19 using routine clinical data for patients attending hospital: development and prospective validation of an artificial intelligence screening test. Lancet Digit Health. 2021 ;3(2):e78-e87. |
| 30 |
He F, Page JH, Weinberg KR, Mishra A. The development and validation of simplified machine learning algorithms to predict prognosis of hospitalized patients with COVID-19: multicenter, retrospective study. J Med Internet Res. 2022; 24(1):e31549.
doi: 10.2196/31549 |
| [1] | Yi Han, Su-cheng Mu, Hai-dong Zhang, Wei Wei, Xing-yue Wu, Chao-yuan Jin, Guo-rong Gu, Bao-jun Xie, Chao-yang Tong. Artificial intelligence computed tomography helps evaluate the severity of COVID-19 patients: A retrospective study [J]. World Journal of Emergency Medicine, 2022, 13(2): 91-97. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
