World Journal of Emergency Medicine ›› 2013, Vol. 4 ›› Issue (1): 20-25.doi: 10.5847/wjem.j.issn.1920-8642.2013.01.004
• Original Articles • Previous Articles Next Articles
Nicola Parenti1( ), Maria Letizia Bacchi Reggiani2, Diego Sangiorgi2, Vito Serventi1, Leopoldo Sarli1
), Maria Letizia Bacchi Reggiani2, Diego Sangiorgi2, Vito Serventi1, Leopoldo Sarli1
Received:2012-10-12
Accepted:2013-01-20
Online:2013-03-15
Published:2013-03-15
Contact:
Nicola Parenti
E-mail:nipar71@yahoo.it
Nicola Parenti, Maria Letizia Bacchi Reggiani, Diego Sangiorgi, Vito Serventi, Leopoldo Sarli. Effect of a triage course on quality of rating triage codes in a group of university nursing students:a before-after observational study[J]. World Journal of Emergency Medicine, 2013, 4(1): 20-25.
Add to citation manager EndNote|Ris|BibTeX
URL: http://wjem.com.cn//EN/10.5847/wjem.j.issn.1920-8642.2013.01.004
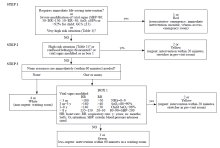
Figure 1.
Triage emergency method algorithm (TEM).
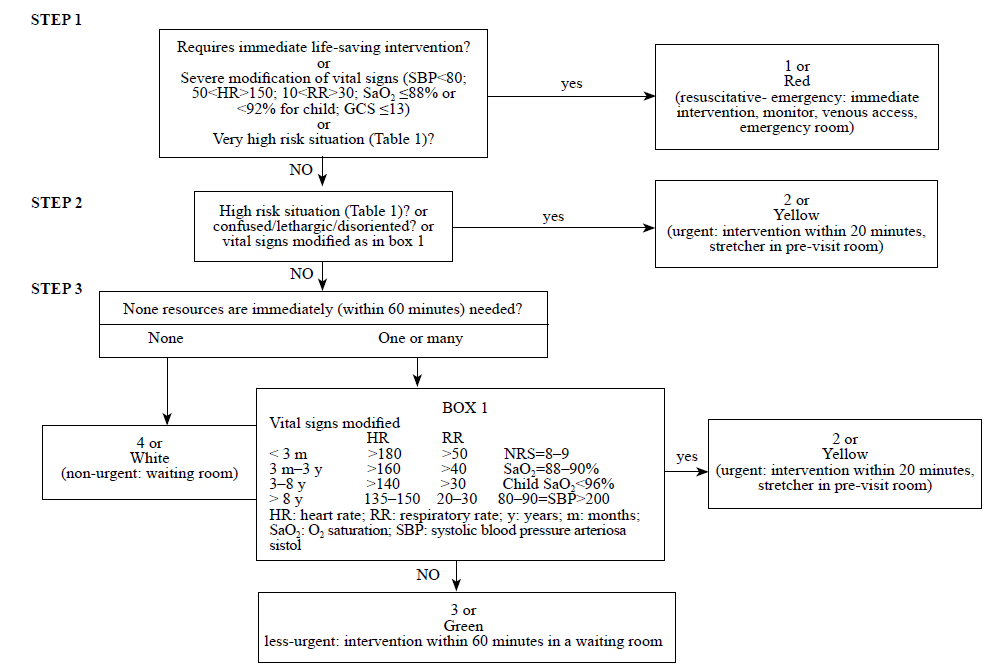
Table 1
Triage emergency method (TEM) patient's chief complaints
| Code | Symptom and situation guide |
|---|---|
| Red (Very high risk situations) | |
| Severe acute pain (NRS=9-10), shock, A.M.I. arrhythmia: actual chest pain with syncope and/or arrhythmia and/or dyspnea; Aphasia and/or numbness <3 h; Dyspnea with wheeze or laryngospasm; Major trauma: penetrating injury, severe facial trauma or cranial trauma with GCS≤ 14, thoracic traumawith volet or dyspnea, abdominal trauma with SBP≤90 mmHg, rachis trauma with sensitive-motor deficit, amputation of long bones, open fractures of long bones, 2nd or 3rd degree skin burns (>30% adult or >20% babies), eyes or airway burns, RTS≤ 10; Multiple trauma with major mechanisms (fall from 5 meters; ejection outside a vehicle; or pedestrian run down; age < 5 years; Severe intoxication (quantity or kind of substance or substance unknown) with dysphonia, dysphagia, chest or abdominal pain. Status epilepticus; Headache with altered level of consciousness or meningism, seizures or syncope; Hematemesis or other severe haemorrhage in action; Severe allergic reactions with dyspnea, dysphonia or severe hypotension; Emergency delivery; eclampsia, severe vaginal bleeding; Children: severe dehydration, headache with GCS ≤14 or lethargy or hypotonia, abuse. | |
| Yellow (High risk situations) | |
| Cardiac: chest pain ≤6 h, syncope, arrhythmia, limbs ischemia, hypertension crisis (SBP >200 mmHg), unstable hypotension (SBP<100 mmHg); Pneumology: mild dyspnea (SaO2 88%-92%); Abdomen: acute abdominal pain, vomit and diarrhea with dehydration, hypovolemia (hypotension-tachycardia), hematemesis, melena, severe rectal bleeding in action; Neurology: headache or with SBP > 200 mmHg, headache after cranial trauma if anticoagulants. Consciousness alterations (agitation, drowsiness, acute confusion), GCS 8-14, aphasia or sensitive-motor deficit <3 h, convulsions. Alcohol or drug abuse. Severe dizziness/vertigo or with headache or motor deficit. Moderate pain (NRS=7-8); Minor intoxication, severe allergic reactions (extensive nettle rash, dysphonia, angioedema, multiple hymenoptera stings in history of anaphylaxis); Infections: fever with lethargy, severe infection (rash or purpura), temperature >39 °C, fever in immunodeficiency; Trauma: concussive cranial trauma or anticoagulants, long bones, dislocation, bone deformation, open fractures, severe lacerations, crush syndrome, limb trauma without pulse, multiple trauma, major dynamic; Acute lumbar pain (if age > 40 yrs or in case of hypertension); severe glycemic failure in diabetes (40 mg/dL < glycemia >300 mg/dL); sexual assault, severe or painful haemorrhage or mild but persistent in anticoagulants or hypertension crisis; Renal-genitourinary: scrotum pain, anuria or oliguria; Gynaecology and obstetrics: vaginal bleeding in the elderly or pregnancy with pain; delivery with active contractions <5 min; pre-eclampsia; pelvic pain. Eye injury with alkali or acid, visual deficit; psychiatric symptoms in patient suffering from mental illness. Severe or mild haemorrhage (any cause); Child: Newborn < 3 months; moderate dehydration, severe vomiting or diarrhea. Recent trauma <12 h.; neonatal crying, recent convulsion. | |
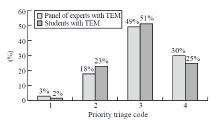
Figure 2.
Urgency category assigned by students and experted nurses.
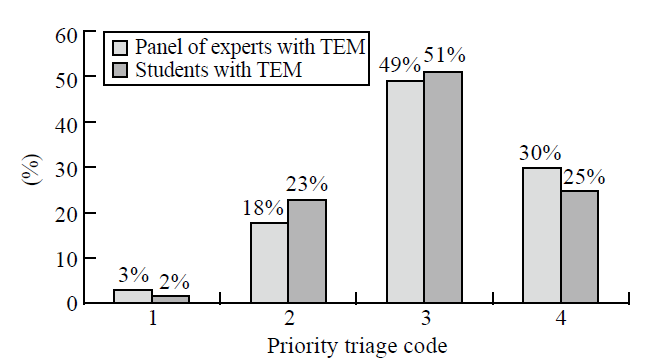
Table 2
Comparison of inter-rater reliability of the students before and after the TEM course
| Variables | Before course (without TEM) | After course (with TEM) | Reference standard (with TEM) |
|---|---|---|---|
| K inter weighted (95%CI) | 0, 42 (0, 37-0, 46) | 0, 61 (0, 56-0, 67) | 0, 75 (0, 71-0, 79) |
| Complete agreement (n, %) | 0 | 0 | 35/105 (33) |
| Complete disagreement (n, %) | 103/105 (98) | 67/105 (64) | 1/105 (2) |
Table 3
The sensitivity and specificity of the students using TEM to predict the reference standard's triage code and admission status
| Variables | Reference standard | Admission status |
|---|---|---|
| Sensitivity (95%CI) | 81% (68-95) | 86% (60-100) |
| Specificity (95%CI) | 80% (66-94) | 87% (78-96) |
| Accuracy (95%CI) | 81% (71-90) | 87% (78-95) |
| Positive predictive value (95%CI) | 81% (68-95) | 46% (19-73) |
| Negative predictive value (95%CI) | 80% (66-94) | 98% (94-100) |
| 1 | Thompson J, Dains J. Comprehensive triage. 1982. Reston Publishing Company Inc. |
| 2 | Standards Committee Council. National Triage Scale. Emerg Med 1994; 6:145-146. |
| 3 |
Beveridge R. CAEP issues. The Canadian triage and Acuity Scale: A new and critical element in health care reform. Canadian Association of Emergency Physician. J Emerg Med 1998; 16:507-511.
pmid: 9610988 |
| 4 | Manchester Triage Group. Emergency Triage. Plymouth, UK: BMJ Publishing Group; 1977. |
| 5 |
Wuerz RC, Milne LW, Eitel DR, Travers D, Gilboy N. Reliability and validity of a new five-level triage instrument. Acad Emerg Med 2000; 7:236-242.
pmid: 10730830 |
| 6 |
Eitel DR, Travers DA, Rosenau AM, Gilboy N, Wuerz RC. The Emergency Severity Index Triage Algorithm Version 2 is reliable and valid. Acad Emerg Med 2003; 10:1070-1080.
pmid: 14525740 |
| 7 | Tanabe P, Gimbel R, Yarnold PR, Kyriacou DN, Adams JG. Reliability and validity of scores on the Emergency Severity Index Version 3. Acad Emerg Med 2004; 11:59-65. |
| 8 |
Wuerz RC, Travers D, Gilboy N, Eitel DR, Rosenau A, Yazhari R. Implementation and refinement of the emergency severity index. Acad Emerg Med 2001; 8:170-176.
pmid: 11157294 |
| 9 | "Triage intraospedaliero nel sistema dell'emergenza-urgenza sanitaria". Gazzetta Ufficiale n. 285 del 7712/2001. www.gazzettaufficiale.it. |
| 10 | Parenti N, Ferrara L, Bacchi Reggiani ML, Sangiorgi D, Lenzi T. Reliability and validity of two four-level emergency triage systems. Eur J Emerg Med 2009; 16:115-120. |
| 11 | Nicola Parenti, Maria Letizia Bocchi Reggiani, Tiziano Lenzi. Affidabilità e validità di un metodo di triage di Pronto Soccorso a 4 codici di priorità. Emerg Care J 2008; 5:30-33. |
| 12 | Parenti N, Manfredi R, Bacchi Reggiani ML, Sangiorgi D, Lenzi T. Reliability and validity of an Italian four-level emergency triage system. Emerg Med J 2010; 27:495-498. |
| 13 |
Fernandes CM, Tanabe P, Gilboy N, Johnson LA, McNair RS, Rosenau AM, et al. Five-level triage: a report from the ACEP/ENA Five-level Triage Task Force. J Emerg Nurs 2005; 31:39-50.
pmid: 15682128 |
| 14 | Worster A, Gilboy N, Fernandes CM, Eitel D, Eva K, Geisler R, et al. Assessment of inter-observer reliability of two five-level triage and acuity scales: a randomized controlled trial. Can J Emerg Med 2004; 6:240-245. |
| 15 | Storm-Versloot MN, Ubbink DT, China Choi V, Luitse JS. Observer agreement of the Manchester Triage System and the Emergency Severity Index: a simulation study. Emerg Med J 2009; 26:556-560. |
| 16 |
van der Wulp I, Schrijvers AJ, van Stel HF. Predicting admission and mortality with the Emergency Severity Index and the Manchester Triage System: a retrospective observational study. Emerg Med J 2009; 26:506-509.
pmid: 19546272 |
| 17 |
Twomey M, Wallis L, Myers JE. Limitations in validating emergency department triage scales. Emerg Med J 2007; 24:477-479.
pmid: 17582037 |
| [1] | Lori Stolz, Elaine Situ-LaCasse, Josie Acuña, Matthew Thompson, Nicolaus Hawbaker, Josephine Valenzuela, Uwe Stolz, Srikar Adhikari. What is the ideal approach for emergent pericardiocentesis using point-of-care ultrasound guidance? [J]. World Journal of Emergency Medicine, 2021, 12(3): 169-173. |
| [2] | Janett Kreutziger, Philip Puchner, Stefan Schmid, Wolfgang Mayer, Harald Prossliner, Wolfgang Lederer. Accuracy of training blood volume quantification using a visual estimation tool [J]. World Journal of Emergency Medicine, 2021, 12(3): 174-178. |
| [3] | Kasım Turgut, Erdal Yavuz, Mine Kayacı Yıldız, Mehmet Kaan Poyraz. Violence toward emergency physicians: A prospective-descriptive study [J]. World Journal of Emergency Medicine, 2021, 12(2): 111-116. |
| [4] | Marin Pavlov, Lucija Klobučar, Iva Klobučar, Kristina Žgela, Vesna Degoricija. Does shifting to professional emergency department staffing affect the decision for chest radiography? [J]. World Journal of Emergency Medicine, 2021, 12(2): 87-92. |
| [5] | Hady Zgheib, Aline El Zakhem, Cynthia Wakil, Mohamad Ali Cheaito, Rola Cheaito, Antoine Finianos, Ralphe Bou Chebl, Rima Kaddoura, Nader Al Souky, Imad El Majzoub. Role of urine studies in asymptomatic febrile neutropenic patients presenting to the emergency department [J]. World Journal of Emergency Medicine, 2021, 12(2): 99-104. |
| [6] | William Gilliam, Jackson F. Barr, Brandon Bruns, Brandon Cave, Jordan Mitchell, Tina Nguyen, Jamie Palmer, Mark Rose, Safura Tanveer, Chris Yum, Quincy K. Tran. Factors associated with refractory pain in emergency patients admitted to emergency general surgery [J]. World Journal of Emergency Medicine, 2021, 12(1): 12-17. |
| [7] | Chang Pan, Jiao-jiao Pang, Kai Cheng, Feng Xu, Yu-guo Chen. Trends and challenges of emergency and acute care in Chinese mainland: 2005-2017 [J]. World Journal of Emergency Medicine, 2021, 12(1): 5-11. |
| [8] | Rebekah Shaw, Erica Popovsky, Alyssa Abo, Marni Jacobs, Nicole Herrera, James Chamberlain, Andrea Hahn. Improving antibiotic prescribing in the emergency department for uncomplicated community-acquired pneumonia [J]. World Journal of Emergency Medicine, 2020, 11(4): 199-205. |
| [9] | Hai-jiang Zhou, Tian-fei Lan, Shu-bin Guo. Outcome prediction value of National Early Warning Score in septic patients with community-acquired pneumonia in emergency department: A single-center retrospective cohort study [J]. World Journal of Emergency Medicine, 2020, 11(4): 206-215. |
| [10] | Chuan-qi Ding, Yu-ping Zhang, Yu-wei Wang, Min-fei Yang, Sa Wang, Nian-qi Cui, Jing-fen Jin. Death and do-not-resuscitate order in the emergency department: A single-center three-year retrospective study in the Chinese mainland [J]. World Journal of Emergency Medicine, 2020, 11(4): 231-237. |
| [11] | Guo-xiong Chen, Hong-na Wang, Jin-lin Zou, Xiao-xu Yuan. Effects of intracoronary injection of nicorandil and tirofiban on myocardial perfusion and short-term prognosis in elderly patients with acute ST-segment elevation myocardial infarction after emergency PCI [J]. World Journal of Emergency Medicine, 2020, 11(3): 157-163. |
| [12] | Maybritt I. Kuypers, Adinda Klijn, Nieke E. Mullaart-Jansen, Frans B. Plötz. Availability and quality of procedural sedation and analgesia in emergency departments without emergency physicians: A national survey in the Netherlands [J]. World Journal of Emergency Medicine, 2020, 11(2): 69-73. |
| [13] | Emily Shao, Chantelle Judge, Erin McMeniman, Tina Bazianas, Rob Eley. Presenting patterns of dermatology conditions to an Australian emergency department [J]. World Journal of Emergency Medicine, 2020, 11(2): 74-78. |
| [14] | Zhenghong Liu, Mingwei Ng, Dinesh V. Gunasekeran, Huihua Li, Kishanti Ponampalam, R Ponampalam. Mobile technology: Usage and perspective of patients and caregivers presenting to a tertiary care emergency department [J]. World Journal of Emergency Medicine, 2020, 11(1): 5-11. |
| [15] | Samantha Shwe, Lauren Witchey, Shadi Lahham, Ethan Kunstadt, Inna Shniter, John C. Fox. Retrospective analysis of eFAST ultrasounds performed on trauma activations at an academic level-1 trauma center [J]. World Journal of Emergency Medicine, 2020, 11(1): 12-17. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
