World Journal of Emergency Medicine ›› 2020, Vol. 11 ›› Issue (4): 199-205.doi: 10.5847/wjem.j.1920-8642.2020.04.001
Special Issue: Survey on Emergency Medicine
• Original Article • Next Articles
Rebekah Shaw1( ), Erica Popovsky1, Alyssa Abo2,3, Marni Jacobs4, Nicole Herrera4, James Chamberlain2,3, Andrea Hahn3,5
), Erica Popovsky1, Alyssa Abo2,3, Marni Jacobs4, Nicole Herrera4, James Chamberlain2,3, Andrea Hahn3,5
Received:2019-07-17
Accepted:2020-03-20
Online:2020-10-01
Published:2020-10-01
Contact:
Rebekah Shaw
E-mail:rebekash@med.umich.edu
Rebekah Shaw, Erica Popovsky, Alyssa Abo, Marni Jacobs, Nicole Herrera, James Chamberlain, Andrea Hahn. Improving antibiotic prescribing in the emergency department for uncomplicated community-acquired pneumonia[J]. World Journal of Emergency Medicine, 2020, 11(4): 199-205.
Add to citation manager EndNote|Ris|BibTeX
URL: http://wjem.com.cn//EN/10.5847/wjem.j.1920-8642.2020.04.001
Table 1
Characteristics of survey respondents and overall response rates
| Levels of training | n (%) | Response rates |
|---|---|---|
| Pediatrics resident Emergency associate PEM fellow PEM attending Total | 40 (48.8) 8 (9.8) 9 (11.0) 25 (30.5) 82 (100.0) | 30.7% (40/130) 32.0% (8/25) 75.0% (9/12) 58.1% (25/43) 39.0% (82/210) |
Figure 1.
Survey frequency of case-based ampicillin versus observed ampicillin use. The P-value determined using Chi-square; other antibiotics included azithromycin (n=1, survey), cefdinir (n=1, survey), and ampicillin/sulbactam (n=3, pre-CPG).
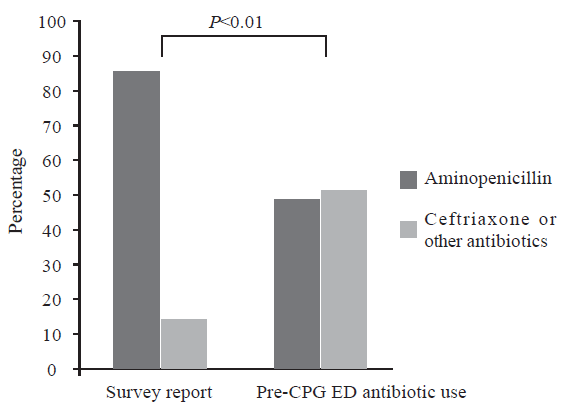

Figure 2.
Flow diagram of selection of eligible subjects for study between January 2015 and February 2017.
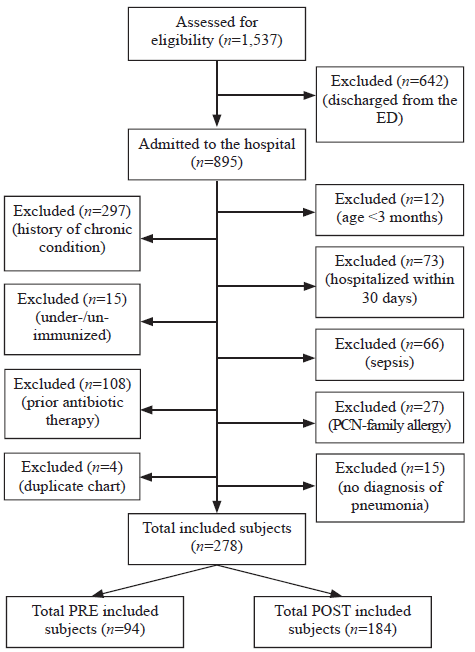
Table 2
Characteristics of enrolled patients pre- and post-CPG implementation, n (%)
| Variables | Pre-implementation (n=94) | Post-implementation (n=184) |
|---|---|---|
| Age (months) (mean) | 21.5 | 36.3 |
| 3 - <13 | 37 (39.4) | 44 (23.9) |
| 13 - <61 | 55 (58.5) | 111 (60.3) |
| ≥61 | 2 (2.1) | 29 (15.8) |
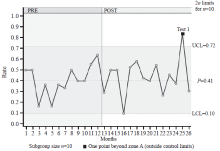
Figure 3.
Rates of ampicillin prescribing by month pre- and post-CPG implementation. UCL: upper control limit; LCL: lower control limit; CPG: clinical practice guideline.
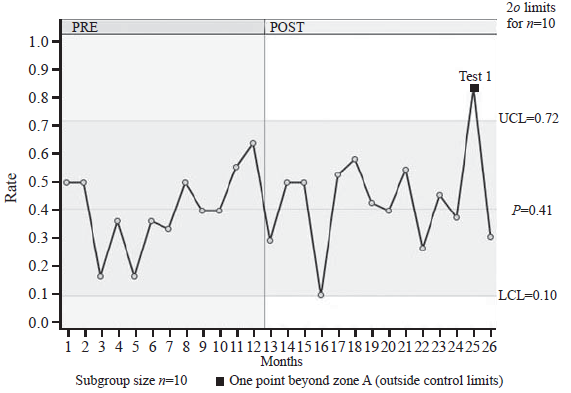
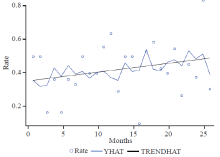
Figure 4.
Trend-analysis of IV ampicillin use over time. YHAT: the full model prediction values; TRENDHAT: the autocorrelation corrected regression line of the structural predicted values; the trend was not statistically significant (P=0.40, Mann-Kendall test).

Table 3
Characteristics of patients in POST group prescribed ampicillin versus ceftriaxone
| Variables | Ampicillin (n=84) | Ceftriaxone (n=97) | Odds ratio (OR), ampicillin prescribed, 95% CI |
|---|---|---|---|
| Age, n (%) | |||
| 3 - <13 months | 16 (19.1) | 28 (28.9) | 0.58 (0.29-1.17) |
| 13 - <61 months | 55 (65.5) | 54 (55.7) | 1.51 (0.83-2.76) |
| ≥61 months | 13 (15.5) | 15 (15.5) | 1.00 (0.45-2.25) |
| Vitals at presentation, n (%) | |||
| Fever (temperature ≥38 oC); missing | 36 (43.4); 1 | 47 (49.5); 2 | 0.78 (0.43-1.41) |
| Tachycardiaa; missing | 77 (91.7); 0 | 80 (83.3); 1 | 2.20 (0.86-5.64) |
| Tachypneaa | 65 (77.4) | 68 (70.8) | 1.41 (0.72-2.77) |
| Hypoxia (SaO2 <90% and/or FiO2 >21%) | 18 (21.4) | 16 (16.5) | 1.38 (0.65-2.92) |
| Laboratory results, n (%) | |||
| Elevated WBC counta; missing | 13 (30.2); 41 | 18 (26.1); 28 | 1.23 (0.53-2.86) |
| Positive blood culturesb; missing | 0 (0); 69 | 2 (4.1); 48 | NA |
| Positive urine culturesb; missing | 0 (0); 76 | 2 (8.3); 73 | NA |
| pH <7.32b; missing | 2 (22.2); 75 | 2 (10.5); 78 | NA |
| PCO2 >50 mmHgb; missing | 2 (22.2); 75 | 1 (5.3); 78 | NA |
| Seasons of admission, n (%) (n=181) | |||
| Spring (March - May) | 26 (31.0) | 24 (25.0) | 1.36 (0.71-2.62) |
| Summer (June - August) | 14 (16.7) | 15 (15.6) | 1.09 (0.49-2.42) |
| Fall (September - November) | 15 (17.9) | 21 (21.9) | 0.79 (0.38-1.65) |
| Winter (December - February) | 29 (34.5) | 37 (38.1) | 0.86 (0.47-1.57) |
| 1 |
Milner TL, McCulloh R, Koster M, Biondi E, Hill V, Ralston S. Antibiotic prescribing patterns across continuum of care for children hospitalized with community-acquired pneumonia. Pediatr Emerg Care. 2018; 34(1):e7-10.
doi: 10.1097/PEC.0000000000000598 pmid: 26555311 |
| 2 |
Jain S, Williams DJ, Arnold SR, Ampofo K, Bramley AM, Reed C, et al. Community-acquired pneumonia requiring hospitalization among U.S. children. N Engl J Med. 2015; 372(9):835-45.
doi: 10.1056/NEJMoa1405870 pmid: 25714161 |
| 3 |
Katz SE, Williams DJ. Pediatric community-acquired pneumonia in the United States: changing epidemiology, diagnostic and therapeutic challenges, and areas for future research. Infect Dis Clin North Am. 2018; 32(1):47-63.
doi: 10.1016/j.idc.2017.11.002 pmid: 29269189 |
| 4 |
Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, et al. Management of Community-Acquired Pneumonia in Infants and Children Older than 3 Months of Age: Clinical Practice Guidelines by the Pediatric Infectious Disease Society and the Infectious Disease Society of America. Clin Infect Dis. 2011; 53(7):e25-76.
doi: 10.1093/cid/cir531 |
| 5 |
Shaughnessy EE, Stalets EL, Shah SS. Community-acquired pneumonia in the post 13-valent pneumococcal conjugate vaccine era. Curr Opin Pediatr. 2016; 28(6):786-93.
doi: 10.1097/MOP.0000000000000428 pmid: 27755118 |
| 6 |
Neuman MI, Shah SS, Shaprio DJ, Hersh AL. Emergency department management of childhood pneumonia in the United States prior to publication of national guidelines. Acad Emerg Med. 2013; 20(3):240-6.
doi: 10.1111/acem.12088 |
| 7 |
Williams DJ, Hall M, Shah SS, Parikh K, Tyler A, Neuman MI, et al. Narrow vs. broad-spectrum antimicrobial therapy for children hospitalized with pneumonia. Pediatrics. 2013; 132(5):e1141-8.
doi: 10.1542/peds.2013-1614 pmid: 24167170 |
| 8 |
Williams DJ, Edwards KM, Self WH, Zhu Y, Ampofo K, Pavia AT, et al. Antibiotic choice for children hospitalized with pneumonia and adherence to national guidelines. Pediatrics. 2015; 136(1):44-52.
doi: 10.1542/peds.2014-3047 pmid: 26101356 |
| 9 |
Handy LK, Bryan M, Gerber JS, Zaoutis T, Feemster KA. Variability in antibiotic prescribing for community-acquired pneumonia. Pediatrics. 2017; 139(4):e20162331.
doi: 10.1542/peds.2016-2331 pmid: 28270546 |
| 10 |
Thomson J, Ambroggio L, Murtagh Kurowski E, Statile A, Graham C, Courter JD, et al. Hospital outcomes associated with guideline-recommended antibiotic therapy for pediatric pneumonia. J Hosp Med. 2015; 10(1):13-8.
doi: 10.1002/jhm.2265 pmid: 25263758 |
| 11 |
Queen MA, Myers AL, Hall M, Shah SS, Williams DJ, Auger KA, et al. Comparative effectiveness of empiric antibiotics for community-acquired pneumonia. Pediatrics. 2014; 133(1):e23-9.
doi: 10.1542/peds.2013-1773 |
| 12 |
Ambroggio L, Thomson J, Murtagh Kurowski E, Courter J, Statile A, Graham C, et al. Quality improvement methods increase appropriate antibiotic prescribing for childhood pneumonia. Pediatrics. 2013; 131(5):e1623-31.
doi: 10.1542/peds.2012-2635 pmid: 23589819 |
| 13 |
Gerber JS, Prasad PA, Fiks AG, Localio AR, Grundmeier RW, Bell LM, et al. Effect of an outpatient antimicrobial stewardship intervention on broad-spectrum antibiotic prescribing by primary care pediatricians: a randomized trial. JAMA. 2013; 309(22):2345-52.
doi: 10.1001/jama.2013.6287 pmid: 23757082 |
| 14 |
Smith MJ, Kong M, Cambon A, Woods CR. Effectiveness of antimicrobial guidelines for community-acquired pneumonia in children. Pediatrics. 2012; 129(5):e1326-33.
doi: 10.1542/peds.2011-2412 |
| 15 |
Neuman MI, Hall M, Hersh AL, Brogan TV, Parikh K, Newland JG, et al. Influence of hospital guidelines on management of children hospitalized with pneumonia. Pediatrics. 2012; 130(5):e823-30.
doi: 10.1542/peds.2012-1285 pmid: 23090342 |
| 16 |
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap): A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009; 42(2):377-81.
doi: 10.1016/j.jbi.2008.08.010 |
| 17 |
Ross RK, Hersh AL, Kronman MP, Newland JG, Metjian TA, Localio AR, et al. Impact of Infectious Diseases Society of America/Pediatric Infectious Diseases Society guidelines on treatment of community-acquired pneumonia in hospitalized children. Clin Infect Dis. 2014; 58(6):834-8.
doi: 10.1093/cid/ciu013 |
| 18 |
Donà D, Zingarella S, Gastaldi A, Lundin R, Perilongo G, Frigo AC, et al. Effects of clinical pathway implementation on antibiotic prescriptions for pediatric community-acquired pneumonia. PLoS One. 2018; 13(2):e0193581.
doi: 10.1371/journal.pone.0193581 pmid: 29489898 |
| [1] | Lori Stolz, Elaine Situ-LaCasse, Josie Acuña, Matthew Thompson, Nicolaus Hawbaker, Josephine Valenzuela, Uwe Stolz, Srikar Adhikari. What is the ideal approach for emergent pericardiocentesis using point-of-care ultrasound guidance? [J]. World Journal of Emergency Medicine, 2021, 12(3): 169-173. |
| [2] | Kasım Turgut, Erdal Yavuz, Mine Kayacı Yıldız, Mehmet Kaan Poyraz. Violence toward emergency physicians: A prospective-descriptive study [J]. World Journal of Emergency Medicine, 2021, 12(2): 111-116. |
| [3] | Marin Pavlov, Lucija Klobučar, Iva Klobučar, Kristina Žgela, Vesna Degoricija. Does shifting to professional emergency department staffing affect the decision for chest radiography? [J]. World Journal of Emergency Medicine, 2021, 12(2): 87-92. |
| [4] | Hady Zgheib, Aline El Zakhem, Cynthia Wakil, Mohamad Ali Cheaito, Rola Cheaito, Antoine Finianos, Ralphe Bou Chebl, Rima Kaddoura, Nader Al Souky, Imad El Majzoub. Role of urine studies in asymptomatic febrile neutropenic patients presenting to the emergency department [J]. World Journal of Emergency Medicine, 2021, 12(2): 99-104. |
| [5] | William Gilliam, Jackson F. Barr, Brandon Bruns, Brandon Cave, Jordan Mitchell, Tina Nguyen, Jamie Palmer, Mark Rose, Safura Tanveer, Chris Yum, Quincy K. Tran. Factors associated with refractory pain in emergency patients admitted to emergency general surgery [J]. World Journal of Emergency Medicine, 2021, 12(1): 12-17. |
| [6] | Hai-jiang Zhou, Tian-fei Lan, Shu-bin Guo. Outcome prediction value of National Early Warning Score in septic patients with community-acquired pneumonia in emergency department: A single-center retrospective cohort study [J]. World Journal of Emergency Medicine, 2020, 11(4): 206-215. |
| [7] | Chuan-qi Ding, Yu-ping Zhang, Yu-wei Wang, Min-fei Yang, Sa Wang, Nian-qi Cui, Jing-fen Jin. Death and do-not-resuscitate order in the emergency department: A single-center three-year retrospective study in the Chinese mainland [J]. World Journal of Emergency Medicine, 2020, 11(4): 231-237. |
| [8] | Zhong-shu Kuang, Yi-lin Yang, Wei Wei, Jian-li Wang, Xiang-yu Long, Ke-yong Li, Chao-yang Tong, Zhan Sun, Zhen-ju Song. Clinical characteristics and prognosis of community-acquired pneumonia in autoimmune disease-induced immunocompromised host: A retrospective observational study [J]. World Journal of Emergency Medicine, 2020, 11(3): 145-151. |
| [9] | Maybritt I. Kuypers, Adinda Klijn, Nieke E. Mullaart-Jansen, Frans B. Plötz. Availability and quality of procedural sedation and analgesia in emergency departments without emergency physicians: A national survey in the Netherlands [J]. World Journal of Emergency Medicine, 2020, 11(2): 69-73. |
| [10] | Emily Shao, Chantelle Judge, Erin McMeniman, Tina Bazianas, Rob Eley. Presenting patterns of dermatology conditions to an Australian emergency department [J]. World Journal of Emergency Medicine, 2020, 11(2): 74-78. |
| [11] | Zhenghong Liu, Mingwei Ng, Dinesh V. Gunasekeran, Huihua Li, Kishanti Ponampalam, R Ponampalam. Mobile technology: Usage and perspective of patients and caregivers presenting to a tertiary care emergency department [J]. World Journal of Emergency Medicine, 2020, 11(1): 5-11. |
| [12] | Wirachin Hoonpongsimanont, Preet Kaur Sahota, Yanjun Chen, Maria Nguyen, Christine Louis, Jonathan Pena, Andrew Wong, Maxwell Jen. Emergency department patient experience: Same location, same provider, different scores by different survey methods [J]. World Journal of Emergency Medicine, 2019, 10(3): 138-144. |
| [13] | Chang Pan, Xiao-ran Huang, Jiao-jiao Pang, Kai Cheng, Feng Xu, Yu-guo Chen. Trends in mortality of emergency departments patients in China [J]. World Journal of Emergency Medicine, 2019, 10(3): 152-155. |
| [14] | Rakesh Gupta, Isaac Siemens, Sam Campbell. The use of outcome feedback by emergency medicine physicians: Results of a physician survey [J]. World Journal of Emergency Medicine, 2019, 10(1): 14-18. |
| [15] | Elaine Situ-LaCasse, Ryan W. Grieger, Stephen Crabbe, Anna L. Waterbrook, Lucas Friedman, Srikar Adhikari. Utility of point-of-care musculoskeletal ultrasound in the evaluation of emergency department musculoskeletal pathology [J]. World Journal of Emergency Medicine, 2018, 9(4): 262-266. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
