World Journal of Emergency Medicine ›› 2015, Vol. 6 ›› Issue (2): 147-152.doi: 10.5847/wjem.j.1920-8642.2015.02.011
• Original Articles • Previous Articles Next Articles
Xue-zhong Xing, Yong Gao( ), Hai-jun Wang, Shi-ning Qu, Chu-lin Huang, Hao Zhang, Hao Wang, Qing-ling Xiao, Ke-lin Sun
), Hai-jun Wang, Shi-ning Qu, Chu-lin Huang, Hao Zhang, Hao Wang, Qing-ling Xiao, Ke-lin Sun
Received:2014-06-06
Accepted:2014-12-22
Online:2015-06-15
Published:2015-06-15
Contact:
Yong Gao
E-mail:2354839907@qq.com
Xue-zhong Xing, Yong Gao, Hai-jun Wang, Shi-ning Qu, Chu-lin Huang, Hao Zhang, Hao Wang, Qing-ling Xiao, Ke-lin Sun. Effect of sedation on short-term and long-term outcomes of critically ill patients with acute respiratory insufficiency[J]. World Journal of Emergency Medicine, 2015, 6(2): 147-152.
Add to citation manager EndNote|Ris|BibTeX
URL: http://wjem.com.cn//EN/10.5847/wjem.j.1920-8642.2015.02.011
Table 1
Univariate analysis of risk factors of in-hospital death for patients receiving ventilation more than 48 hours
| Variables | Alive (n=82) | Dead (n=9) | t/χ2 | Pvalue |
|---|---|---|---|---|
| Age (years) | 61.12±13.64 | 68.22±12.49 | -1.493 | 0.139 |
| Male (n, %) | 60 (73.2) | 5 (55.6) | 1.233 | 0.267 |
| Type of admission(n, %) | 5.160 | 0.023 | ||
| Elective | 31 (37.8) | 0 (0) | ||
| Emergency | 51 (62.2) | 9 (100) | ||
| APACHE II score on admission | 13.20±5.58 | 17.11±10.04 | -1.150 | 0.281 |
| SOFA score on admission | 3.36±2.50 | 6.00±2.92 | -2.963 | 0.004 |
| Sepsis (n, %) | 28 (34.1) | 7 (77.8) | 6.523 | 0.011 |
| Shock (n, %) | 22 (26.8) | 6 (66.7) | 6.042 | 0.014 |
| Duration of ventilation (days) | 5.34±5.84 | 12.22±12.72 | -1.605 | 0.145 |
| ALI/ARDS (n, %) | 20 (24.4) | 4 (44.4) | 1.680 | 0.195 |
| Acute kidney injury (n, %) | 8 (9.8) | 0 (0) | 0.963 | 0.327 |
| Sedation (n, %) | 6.042 | 0.014 | ||
| No | 60 (73.2) | 3 (33.3) | ||
| Yes | 22 (26.8) | 6 (66.7) |
Table 2
Multivariate analysis of predictors of in-hospital death
| Variables | B | SE | Wald | RR (95%CI) | Pvalue |
|---|---|---|---|---|---|
| SOFA | 0.304 | 0.130 | 5.483 | 1.355 (1.051-1.747) | 0.019 |
| Sedation | 1.612 | 0.787 | 4.195 | 5.015 (1.072-23.459) | 0.041 |
| Constant | -4.350 | 0.962 | 20.446 | 0.013 |
Table 3
Comparison of short-term outcome of patients who received sedation or not
| Variables | Sedation group (n=28) | Non-sedation group (n=63) | t/χ2 value | P value |
|---|---|---|---|---|
| Age (years) | 61.6±15.0 | 61.9±13.1 | 0.084 | 0.933 |
| Male (n, %) | 20 (71.4) | 45 (71.4) | 0.000 | 1.000 |
| Type of admission (n, %) | 4.731 | 0.030 | ||
| Elective | 5 (17.9) | 26 (41.3) | ||
| Emergency | 23 (82.1) | 37 (58.7) | ||
| APACHE II score on admission | 13.82±6.70 | 13.48±6.01 | -0.244 | 0.808 |
| SOFA score on admission | 4.30±2.79 | 3.33±2.55 | -1.596 | 0.114 |
| Sepsis (n, %) | 19 (67.9) | 16 (25.4) | 14.766 | <0.001 |
| Shock (n, %) | 9 (32.1) | 19 (30.2) | 0.036 | 0.850 |
| Duration of ventilation (days) | 8.96±8.17 | 4.71±6.07 | -2.762 | 0.007 |
| ICU mortality (n, %) | 3 (10.7) | 3 (4.8) | 1.115 | 0.291 |
| ICU length of stay (days) | 11.07±8.25 | 6.33±6.14 | -3.046 | 0.003 |
| In-hospital mortality (n, %) | 6 (21.4) | 3 (4.8) | 6.042 | 0.014 |
| Hospital length of stay (days) | 33.36±16.13 | 26.67±12.64 | -2.120 | 0.037 |

Figure 1.
Long-term outcomes of patients who had received sedation or no sedation

Table 4
Short-term outcomes of patients who had received different type of sedation
| Variables | Deep sedation (n=7) | Daily interruption and/or light sedation (n=21) | t/χ2 value | P value |
|---|---|---|---|---|
| Duration of ventilation (days) | 12.86±13.38 | 7.67±5.42 | 0.999 | 0.353 |
| APACHE II score on admission | 14.00±5.07 | 13.76±7.27 | 0.080 | 0.937 |
| SOFA score on admission | 5.86±3.13 | 3.75±2.51 | 1.795 | 0.085 |
| ICU mortality (n, %) | 2 (28.6) | 1 (4.8) | 3.111 | 0.078 |
| ICU length of stay (days) | 14.71±12.23 | 9.86±6.38 | 1.006 | 0.347 |
| In-hospital mortality (n, %) | 4 (57.1) | 2 (9.5) | 7.071 | 0.008 |
| Hospital length of stay (days) | 42.00±13.87 | 30.48±16.08 | 1.693 | 0.102 |
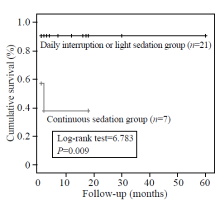
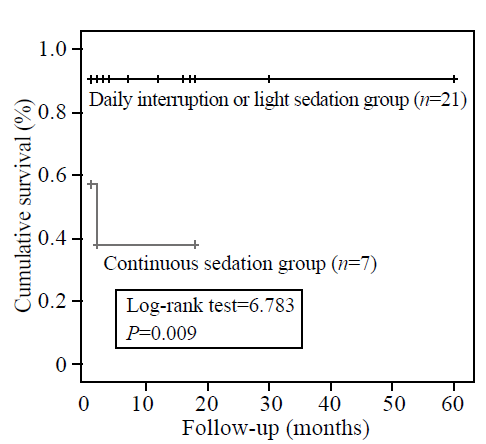
Figure 2.
Long-term outcomes of the patients who had received different types of sedation
| 1 | Franca SA, Toufen C Jr, Hovnanian AL, Albuquerque AL, Borges ER, Pizzo VR, et al. The epidemiology of acute respiratory failure in hospitalized patients: a Brazilian prospective cohort study. J Crit Care 2011; 26: 330.e1-8. |
| 2 |
Xing XZ, Gao Y, Wang HJ, Yang QH, Huang CL, Qu SN, et al. Risk factors and prognosis of critically ill cancer patients with postoperative acute respiratory insufficiency. World J Emerg Med 2013; 4:43-47.
pmid: 25215091 |
| 3 | Thille AW, Contou D, Fragnoli C, Córdoba-Izquierdo A, Boissier F, Brun-Buisson C. Non-invasive ventilation for acute hypoxemic respiratory failure: intubation rate and risk factors. Crit Care 2013; 17:R269. |
| 4 |
Yu KY, Zhao L, Chen Z, Yang M. Noninvasive positive pressure ventilation for the treatment of acute respiratory distress syndrome following esophagectomy for esophageal cancer: a clinical comparative study. J Thorac Dis 2013; 5:777-782.
doi: 10.3978/j.issn.2072-1439.2013.09.09 pmid: 24409355 |
| 5 | Reade MC, Finfer S. Sedation and delirium in the intensive care unit. N Engl J Med 2014; 370:444-454. |
| 6 |
Kress JP, Pohlman AS, O'Connor MF, Hall JB. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med 2000; 342:1471-1477.
doi: 10.1056/NEJM200005183422002 pmid: 10816184 |
| 7 |
Treggiari MM, Romand JA, Yanez ND, Deem SA, Goldberg J, Hudson L, et al. Randomized trial of light versus deep sedation on mental health after critical illness. Crit Care Med 2009; 37:2527-2534.
pmid: 19602975 |
| 8 |
Strøm T, Martinussen T, Toft P. A protocol of no sedation for critically ill patients receiving mechanical ventilation: a randomised trial. Lancet 2010; 375:475-480.
pmid: 20116842 |
| 9 | Ramsay MA, Savege TM, Simpson BR, Goodwin R. Controlled sedation with alphaxalone-alphadolone. BMJ 1974; 2:656-659. |
| 10 |
Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med 2003; 31:1250-1256.
doi: 10.1097/01.CCM.0000050454.01978.3B pmid: 12682500 |
| 11 | Xing XZ, Wang HJ, Huang CL, Yang QH, Qu SN, Zhang H, et al. Prognosis of patients with shock receiving vasopressors. World J Emerg Med 2013; 4:59-62. |
| 12 |
Mehta RL, Kellum JA, Shah SV, Molitoris BA, Ronco C, Warnock DG, et al. Acute Kidney Injury Network: report of an initiative to improve outcomes in acute kidney injury. Crit Care 2007; 11:R31.
pmid: 17331245 |
| 13 |
Chinese Society of Critical Care Medicine; Chinese Medical Association. Guidelines for management of acute lung injury/acute respiratory distress syndrome: an evidence-based update by the Chinese Society of Critical Care Medicine (2006). Zhongguo Wei Zhong Bing Ji Jiu Yi Xue 2006; 18:706-710. [Article in Chinese]
pmid: 17166345 |
| 14 |
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med 1985; 13:818-829.
pmid: 3928249 |
| 15 |
Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med 1996; 22:707-710.
doi: 10.1007/BF01709751 pmid: 8844239 |
| 16 |
Burry L, Rose L, McCullagh IJ, Fergusson DA, Ferguson ND, Mehta S. Daily sedation interruption versus no daily sedation interruption for critically ill adult patients requiring invasivemechanical ventilation. Cochrane Database Syst Rev 2014; 7: CD009176.
pmid: 32691879 |
| 17 | Shehabi Y, Bellomo R, Reade MC, Bailey M, Bass F, Howe B, et al. Early intensive care sedation predicts long-term mortality in ventilated critically ill patients. Am J Respir Crit Care Med 2012; 186:724-731. |
| 18 |
Tanaka LM, Azevedo LC, Park M, Schettino G, Nassar AP, Réa-Neto A, et al. Early sedation and clinical outcomes of mechanically ventilated patients: a prospective multicenter cohort study. Crit Care 2014; 18:R156.
pmid: 25047960 |
| [1] | Yu-ming Wang, Yan-jun Zheng, Ying Chen, Yun-chuan Huang, Wei-wei Chen, Ran Ji, Li-li Xu, Zhi-tao Yang, Hui-qiu Sheng, Hong-ping Qu, En-qiang Mao, Er-zhen Chen. Effects of fluid balance on prognosis of acute respiratory distress syndrome patients secondary to sepsis [J]. World Journal of Emergency Medicine, 2020, 11(4): 216-222. |
| [2] | Maybritt I. Kuypers, Adinda Klijn, Nieke E. Mullaart-Jansen, Frans B. Plötz. Availability and quality of procedural sedation and analgesia in emergency departments without emergency physicians: A national survey in the Netherlands [J]. World Journal of Emergency Medicine, 2020, 11(2): 69-73. |
| [3] | Wen-peng Yin, Jia-bao Li, Xiao-fang Zheng, Le An, Huan Shao, Chun-sheng Li. Effect of neutrophil CD64 for diagnosing sepsis in emergency department [J]. World Journal of Emergency Medicine, 2020, 11(2): 79-86. |
| [4] | Shahin Shadnia, Nasim Zaman, Hossein Hassanian-Moghaddam, Hamed Shafaroodi, Mina Padandar, Mohammad Hasan Rezaeizadeh. Prognostic value of cortisol and thyroid function tests in poisoned patients admitted to toxicology ICU [J]. World Journal of Emergency Medicine, 2018, 9(1): 51-55. |
| [5] | Michael Butler, Patrick Froese, Peter Zed, George Kovacs, Robert MacKinley, Kirk Magee, Mary-Lynn Watson, Samuel G. Campbell. Emergency department procedural sedation for primary electrical cardioversion — a comparison with procedural sedations for other reasons [J]. World Journal of Emergency Medicine, 2017, 8(3): 165-169. |
| [6] | Samuel G. Campbell, Kirk D. Magee, Peter J. Zed, Patrick Froese, Glenn Etsell, Alan LaPierre, Donna Warren, Robert R. MacKinley, Michael B. Butler, George Kovacs, David A. Petrie. End-tidal capnometry during emergency department procedural sedation and analgesia: a randomized, controlled study [J]. World Journal of Emergency Medicine, 2016, 7(1): 13-18. |
| [7] | Wei-ping Sun, Guang-xiong Yuan, Yan-juan Hu, Li-zhen Liao, Lin Fu. Effect of low-dose glucocorticoid on corticosteroid insufficient patients with acute exacerbation of chronic obstructive pulmonary disease [J]. World Journal of Emergency Medicine, 2015, 6(1): 34-39. |
| [8] | Kun Chen, Qiu-xiang Zhou, Hong-wei Shan, Wen-fang Li, Zhao-fen Lin. Prognostic value of CD4+CD25+ Tregs as a valuable biomarker for patients with sepsis in ICU [J]. World Journal of Emergency Medicine, 2015, 6(1): 40-43. |
| [9] | Lin Dou, Hong-mei Gao, Ling Lu, Wen-xiu Chang. Bispectral index in predicting the prognosis of patients with coma in intensive care unit [J]. World Journal of Emergency Medicine, 2014, 5(1): 53-56. |
| [10] | Hai-yan Zhang, Cai-jun Wu, Chun-sheng Li. Glycated hemoglobin A1C and diabetes mellitus in critically ill patients [J]. World Journal of Emergency Medicine, 2013, 4(3): 201-204. |
| [11] | Xue-zhong Xing, Yong Gao, Hai-jun Wang, Quan-hui Yang, Chu-lin Huang, Shi-ning Qu, Hao Zhang, Hao Wang, Qing-ling Xiao, Ke-lin Sun. Risk factors and prognosis of critically ill cancer patients with postoperative acute respiratory insufficiency [J]. World Journal of Emergency Medicine, 2013, 4(1): 43-47. |
| [12] | Chun-tao Wu, Zhong-hua Wang, Zhu-qin Li, Lan-feng Wang. Effect of spironolactone on cardiac remodeling after acute myocardial infarction [J]. World Journal of Emergency Medicine, 2013, 4(1): 48-53. |
| [13] | Jonathan Pester, Joseph Robinson, John Prestosh, Suzanne Roozendaal, Rebecca Jeanmonod. Impact of the United States propofol ban on emergency providers' procedural sedation agent choice and patient length of stay [J]. World Journal of Emergency Medicine, 2012, 3(3): 177-181. |
| [14] | He-chen Zhu, Ruo-lan Cao. The relationship between serum levels of uric acid and prognosis of infection in critically ill patients [J]. World Journal of Emergency Medicine, 2012, 3(3): 186-190. |
| [15] | Jun Yin, Yao Chen-ling, Cheng-long Liu, Zhen-ju Song, Chao-yang Tong, Pei-zhi Huang. Association of genetic variants in the IRAK-4 gene with susceptibility to severe sepsis [J]. World Journal of Emergency Medicine, 2012, 3(2): 123-127. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
