World Journal of Emergency Medicine ›› 2015, Vol. 6 ›› Issue (1): 34-39.doi: 10.5847/wjem.j.1920-8642.2015.01.006
• Original Articles • Previous Articles Next Articles
Wei-ping Sun1, Guang-xiong Yuan2, Yan-juan Hu3( ), Li-zhen Liao1, Lin Fu2
), Li-zhen Liao1, Lin Fu2
Received:2014-07-12
Accepted:2015-01-17
Online:2015-03-15
Published:2015-03-15
Contact:
Yan-juan Hu
E-mail:707321845@qq.com
Wei-ping Sun, Guang-xiong Yuan, Yan-juan Hu, Li-zhen Liao, Lin Fu. Effect of low-dose glucocorticoid on corticosteroid insufficient patients with acute exacerbation of chronic obstructive pulmonary disease[J]. World Journal of Emergency Medicine, 2015, 6(1): 34-39.
Add to citation manager EndNote|Ris|BibTeX
URL: http://wjem.com.cn//EN/10.5847/wjem.j.1920-8642.2015.01.006
Table 1
Clinical and biochemical parameters of the AECOPD patients with or without CIRCI
| Baseline data | Patients with CIRCI | Patients without CIRCI |
|---|---|---|
| Cases (male/female) | 63 (50/13) | 322 (255/67) |
| Age (year) | 72.3±16.8# | 58.2±18.9 |
| Shock incidence | 23.8%# | 8.7% |
| PaO2 (mmHg) | 65.7±11.8* | 75.6±12.3 |
| PaCO2 (mmHg) | 47.1±13.4 | 42.5±11.4 |
| Base excess (mmol/L) | 2.5 (-7.5, 8.6) | 2.0 (-8.2, 7.9) |
| pH | 7.43±0.18 | 7.40±0.21 |
| APACHE II (scores) | 17.0±4.8 | 14.3±4.0 |
| CPIS (scores) | 4.8±1.8 | 4.0±1.2 |
| CAPS score (score) | 29.8±7.8 | 25.5±6.5 |
| CRP (mg/L) | 13.4±5.3 | 12.1±4.5 |
| IL-6 (μg/L) | 13.6±7.2 | 14.5±9.1 |
| TNF-α (μg/L) | 25.3±15.7 | 23.1±14.0 |
| PCT (μg/L) | 3.85 (0.25, 8.3) | 3.25 (0.18, 7.1) |
| White blood cells (×109/L) | 14.1±5.4 | 14.7±6.0 |
| Platelet (×109/L) | 168±109 | 159±114 |
| Lactic acid (mmol/L) | 3.2 (1.3, 4.6)* | 2.5 (1.1, 4.0) |
Figure 1.
Effect of glucocorticoid on the survival rate of the corticosteroid insufficient patients with AECOPD.
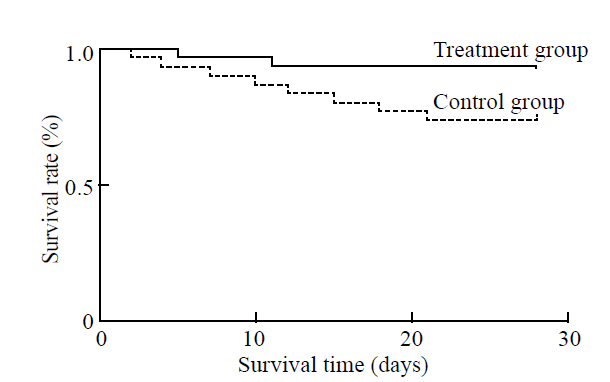
Table 2
Effect of glucocorticoid on prognosis, disease severity and markers of infection and inflammation in the corticosteroid insufficient patients with AECOPD
| Parameters | Control group | Treatment group |
|---|---|---|
| Cases (male/female) | 31 (25/6) | 32 (25/7) |
| Age (years) | 71.8±15.9 | 72.7±17.2 |
| Prevalence baseline shock | 7/31 | 8/32 |
| 28-day non-mechanical ventilation time (days) | 18.3±6.2 | 20.5±5.1 |
| 28-day shock incidence | 11/31 | 8/32 |
| 28-day non-shock time (days) | 18.2±9.5 | 25.8±4.1* |
| 28-day duration of ICU stay (days) | 12.8±6.1 | 10.5±5.3 |
Table 3
Changes of CRP, TNF-α, IL-6 and PCT before and after treatment
| Parameters | Control group | Treatment group | |||
|---|---|---|---|---|---|
| Before | After | Before | After | ||
| PaO2 (mmHg) | 65.3±11.3 | 80.4±12.5* | 65.9±12.2 | 82.5±11.8* | |
| PaCO2 (mmHg) | 47.4±12.8 | 40.3±11.5* | 46.6±12.6 | 37.8±13.7* | |
| BE (mmol/L) | 2.5 (-7.1, 8.5) | 1.3 (-5.7, 6.8) | 2.5 (-7.8, 8.8) | 1.5 (-4.1, 6.5) | |
| pH | 7.44±0.20 | 7.39±0.12 | 7.43±0.17 | 7.40±0.15 | |
| APACHE II | 16.7±4.5 | 12.3±3.2* | 17.2±4.7 | 10.1±2.9* | |
| CPIS score | 4.8±1.9 | 3.1±0.8* | 4.6±1.8 | 3.0±1.2* | |
| CAPS score | 30.1±6.7 | 20.3±5.4* | 29.2±7.0 | 22.0±5.8* | |
| WBC (×109/L) | 14.3±6.2 | 8.3±4.7# | 14.0±5.5 | 11.9±3.5 | |
| Platelet (×109/L) | 165±105 | 158±96 | 170±112 | 161±103 | |
| CRP (mg/L) | 13.2±5.5 | 8.3±3.1# | 13.5±5.9 | 5.1±2.3#Δ | |
| IL-6 (μg/L) | 13.7±7.5 | 11.4±5.6 | 13.1±6.9 | 8.3±3.2#Δ | |
| TNF-α (μg/L) | 26.1±16.2 | 17.5±9.7# | 25.0±14.8 | 10.4±7.8#▲ | |
| PCT (μg/L) | 3.88 (0.25, 8.5) | 2.03 (0.15, 5.1)# | 3.77 (0.21, 8.0) | 1.26 (0.10, 3.2)#▲ | |
| Lactic acid (mmol/L) | 3.4 (1.2, 4.8) | 2.8 (0.8, 3.6) | 3.2 (1.0, 4.5) | 2.7 (1.0, 4.6) |
| 1 |
Marik PE, Pastores SM, Annane D, Meduri GU, Sprung CL, Arlt W, et al. Recommendations for the diagnosis and management of corticosteroid insufficiency in critically ill adult patients: consensus statements from an international task force by the American College of Critical Care Medicine. Crit Care Med 2008; 36:1937-1949.
pmid: 18496365 |
| 2 |
Annane D, Sébille V, Charpentier C, Bollaert PE, François B, Korach JM, et al. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA 2002; 288:862-871.
pmid: 12186604 |
| 3 |
Liu L, Li J, Huang YZ, Liu SQ, Yang CS, Guo FM, et al. The effect of stress dose glucocorticoid on patients with acute respiratory distress syndrome combined with critical illness-related corticosteroid insufficiency. Zhonghua Nei Ke Za Zhi 2012; 51:599-603.
pmid: 23158856 |
| 4 | Schuetz P, Christ-Crain M, Schild U, Süess E, Facompre M, Baty F, et al. Effect of a 14-day course of systemic corticosteroids on the hypothalamic-pituitary-adrenal-axis in patients with acute exacerbation of chronic obstructive pulmonary disease. BMC Pulm Med 2008; 8:1-8. |
| 5 | Zhang YC, Zhang SJ, Teng GL, Tian GL, Xu L, Cao RF, et al. Adrenal insufficiency evaluation by using low-dose ACTH stimulation test in critical illness children. Zhonghua Er Ke Za Zhi 2012,21:472-477. |
| 6 | Chen YC, Lin YH, Chen SH, Chen YC, Chou LF, Chen TJ, et al. Epidemiology of adrenal insufficiency: a nationwide study of hospitalizations in Taiwan from 1996 to 2008. J Chin Med Assoc 2013; 76:140-145. |
| 7 |
Niewoehner DE, Erbland ML, Deupree RH, Collins D, Gross NJ, Light RW, et al. Effect of systemic glucocorticoids on exacerbations of chronic obstructive pulmonary disease. Department of Veterans Affairs Cooperative Study Group. N Engl J Med 1999; 340:1941-1947.
pmid: 10379017 |
| 8 |
Vondracek SF, Hemstreet BA. Is there an optimal corticosteroid regimen for the management of an acute exacerbation of chronic obstructive pulmonary disease? Pharmacotherapy 2006; 26:522-532.
pmid: 16553512 |
| 9 |
He J, Hou XY. The potential contributions of traditional Chinese medicine to emergency medicine. World J Emerg Med 2013; 4:92-97.
pmid: 25215100 |
| 10 |
Huang CJ, Lin HC. Association between adrenal insufficiency and ventilator weaning. Am J Respir Crit Care Med 2006; 173:276-280.
pmid: 16272449 |
| 11 |
Sprung CL, Annane D, Keh D, Moreno R, Singer M, Freivogel K, et al. Hydrocortisone therapy for patients with septic shock. N Engl J Med 2008; 358:111-124.
pmid: 18184957 |
| 12 |
Thomas Z, Fraser GL. An update on the diagnosis of adrenal insufficiency and the use of corticotherapy in critical illness. Ann Pharmacother 2007; 41:1456-1465.
pmid: 17698896 |
| 13 |
Xie J, Yang XY, Shi JD, Deng XQ, Long W. A new inflammation marker of chronic obstructive pulmonary disease-adiponectin. World J Emerg Med 2010; 1:190-195.
pmid: 25214966 |
| 14 |
Liu ZH, Zhang XR, Hu XY, Cheng MY, Xu JY, Du YC. Effect of glucocorticoid on MIP-1α and NF-κb expressing in the lung of rats undergoing mechanical ventilation with a high tidal volume. World J Emerg Med 2011; 2:66-69.
pmid: 25214986 |
| 15 |
Arafah BM. Hypothalamic pituitary adrenal function during critical illness: limitations of current assessment methods. J Clin Endocrinol Metab 2006; 91:3725-3745.
doi: 10.1210/jc.2006-0674 pmid: 16882746 |
| 16 |
Seam N, Meduri GU, Wang H, Nylen ES, Sun J, Schultz MJ, et al. Effects of methylprednisolone infusion on markers of inflammation, coagulation, and angiogenesis in early acute respiratory distress syndrome. Crit Care Med 2012; 40:495-501.
pmid: 21983371 |
| [1] | Yu-ming Wang, Yan-jun Zheng, Ying Chen, Yun-chuan Huang, Wei-wei Chen, Ran Ji, Li-li Xu, Zhi-tao Yang, Hui-qiu Sheng, Hong-ping Qu, En-qiang Mao, Er-zhen Chen. Effects of fluid balance on prognosis of acute respiratory distress syndrome patients secondary to sepsis [J]. World Journal of Emergency Medicine, 2020, 11(4): 216-222. |
| [2] | Wen-peng Yin, Jia-bao Li, Xiao-fang Zheng, Le An, Huan Shao, Chun-sheng Li. Effect of neutrophil CD64 for diagnosing sepsis in emergency department [J]. World Journal of Emergency Medicine, 2020, 11(2): 79-86. |
| [3] | Wei Bi, Yan Sun, Lin-qin Ma, Cai-jun Wu. Predictive role of interleukin-6 and CAT score in mechanical ventilation in patients with chronic obstructive pulmonary disease at the acute exacerbation stage in the emergency department [J]. World Journal of Emergency Medicine, 2020, 11(2): 93-96. |
| [4] | Shahin Shadnia, Nasim Zaman, Hossein Hassanian-Moghaddam, Hamed Shafaroodi, Mina Padandar, Mohammad Hasan Rezaeizadeh. Prognostic value of cortisol and thyroid function tests in poisoned patients admitted to toxicology ICU [J]. World Journal of Emergency Medicine, 2018, 9(1): 51-55. |
| [5] | Ruo Wu, Luo-gen Peng, Hui-min Zhao. Diverse coagulopathies in a rabbit model with different abdominal injuries [J]. World Journal of Emergency Medicine, 2017, 8(2): 141-147. |
| [6] | Jia-jun Xu, Jian-tao Zhen, Li Tang, Qing-ming Lin. Intravenous injection of Xuebijing attenuates acute kidney injury in rats with paraquat intoxication [J]. World Journal of Emergency Medicine, 2017, 8(1): 61-64. |
| [7] | Li-ping Chen, Jun-hui Chen, Ying Chen, Chao Wu, Xiao-hong Yang. Efficacy and safety of glucocorticoids in the treatment of community-acquired pneumonia: A meta-analysis of randomized controlled trials [J]. World Journal of Emergency Medicine, 2015, 6(3): 172-178. |
| [8] | Şükrü Gürbüz, Mustafa Yıldız, Murat Kara, Kürşat Kargün, Mehtap Gürger, Metin Ateşçelik, Ömer Doğan Alataş. Paraoxonase-1 gene in patients with chronic obstructive pulmonary disease investigation Q192R and L55M polymorphisms [J]. World Journal of Emergency Medicine, 2015, 6(3): 201-206. |
| [9] | Xue-zhong Xing, Yong Gao, Hai-jun Wang, Shi-ning Qu, Chu-lin Huang, Hao Zhang, Hao Wang, Qing-ling Xiao, Ke-lin Sun. Effect of sedation on short-term and long-term outcomes of critically ill patients with acute respiratory insufficiency [J]. World Journal of Emergency Medicine, 2015, 6(2): 147-152. |
| [10] | Kun Chen, Qiu-xiang Zhou, Hong-wei Shan, Wen-fang Li, Zhao-fen Lin. Prognostic value of CD4+CD25+ Tregs as a valuable biomarker for patients with sepsis in ICU [J]. World Journal of Emergency Medicine, 2015, 6(1): 40-43. |
| [11] | Lin Dou, Hong-mei Gao, Ling Lu, Wen-xiu Chang. Bispectral index in predicting the prognosis of patients with coma in intensive care unit [J]. World Journal of Emergency Medicine, 2014, 5(1): 53-56. |
| [12] | Hai-yan Zhang, Cai-jun Wu, Chun-sheng Li. Glycated hemoglobin A1C and diabetes mellitus in critically ill patients [J]. World Journal of Emergency Medicine, 2013, 4(3): 201-204. |
| [13] | Peng Sun, Qian Li, Qing Zhang, Li Xu, Ji-yuan Han. Upregulated expression of S100A8 in mice brain after focal cerebral ischemia reperfusion [J]. World Journal of Emergency Medicine, 2013, 4(3): 210-214. |
| [14] | Xue-zhong Xing, Yong Gao, Hai-jun Wang, Quan-hui Yang, Chu-lin Huang, Shi-ning Qu, Hao Zhang, Hao Wang, Qing-ling Xiao, Ke-lin Sun. Risk factors and prognosis of critically ill cancer patients with postoperative acute respiratory insufficiency [J]. World Journal of Emergency Medicine, 2013, 4(1): 43-47. |
| [15] | Chun-tao Wu, Zhong-hua Wang, Zhu-qin Li, Lan-feng Wang. Effect of spironolactone on cardiac remodeling after acute myocardial infarction [J]. World Journal of Emergency Medicine, 2013, 4(1): 48-53. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
