World Journal of Emergency Medicine ›› 2023, Vol. 14 ›› Issue (6): 428-433.doi: 10.5847/wjem.j.1920-8642.2023.094
• Original Article • Previous Articles Next Articles
Won Jae Yoo, Shin Ahn( ), Bora Chae, Won Young Kim
), Bora Chae, Won Young Kim
Received:2023-01-02
Accepted:2023-05-15
Online:2023-11-10
Published:2023-11-01
Contact:
Shin Ahn, Email: Won Jae Yoo, Shin Ahn, Bora Chae, Won Young Kim. Computed tomography coronary angiography after excluding myocardial infarction: high-sensitivity troponin versus risk score-guided approach[J]. World Journal of Emergency Medicine, 2023, 14(6): 428-433.
Add to citation manager EndNote|Ris|BibTeX
URL: http://wjem.com.cn/EN/10.5847/wjem.j.1920-8642.2023.094

Figure 1.
Flow diagram of the study population. CTCA: computed tomography coronary angiography; HEART: history, electrocardiography, age, risk factors, and troponin; CAD: coronary artery disease; hsTnI: high-sensitivity troponin I.
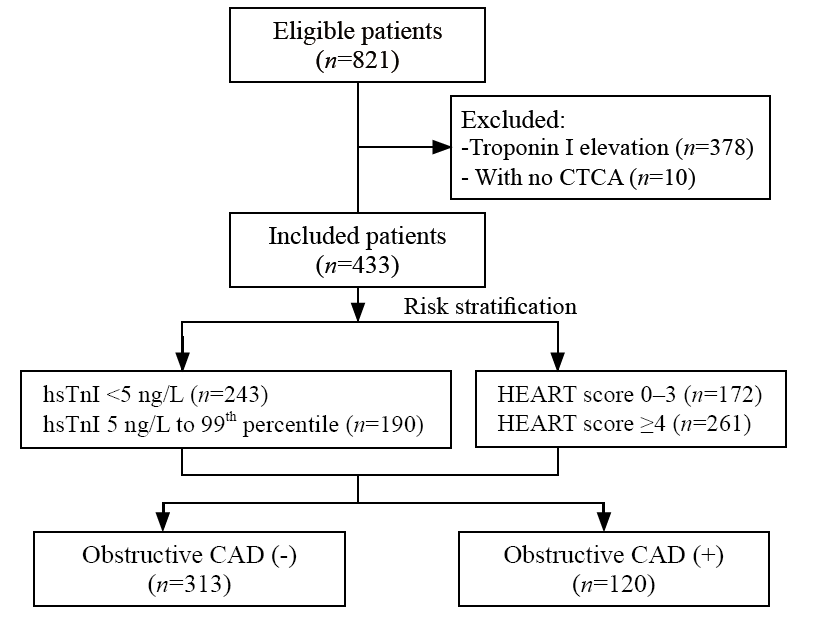
Table 1.
Baseline characteristics of patients stratified by troponin concentration and HEART score
| Variables | Overall (n=433) | hsTnI | HEART score | ||||
|---|---|---|---|---|---|---|---|
| <5 ng/L (n=243) | 5 ng/L to 99th percentile (n=190) | P-value | 0-3 (n=172) | ≥4 (n=261) | P-value | ||
| Sex, male | 252 (58.2) | 131 (53.9) | 121 (63.7) | 0.041 | 95 (55.2) | 157 (60.2) | 0.310 |
| Age, years | 63.9 ± 12.5 | 60.6 ±1.8 | 68.2 ± 12.2 | <0.001 | 55.6 ±11.8 | 69.5 ± 9.6 | <0.001 |
| Risk factors | |||||||
| Hypertension | 215 (49.7) | 106 (43.6) | 109 (57.4) | 0.005 | 54 (31.4) | 161 (61.7) | <0.001 |
| Diabetes mellitus | 97 (22.4) | 50 (20.6) | 47 (24.7) | 0.303 | 19 (11.0) | 78 (29.9) | <0.001 |
| Hyperlipidemia | 135 (31.2) | 78 (32.1) | 57 (30.0) | 0.640 | 48 (27.9) | 87 (33.3) | 0.233 |
| Family history of CAD | 52 (12.0) | 37 (15.2) | 15 (7.9) | 0.020 | 23 (13.4) | 29 (11.1) | 0.479 |
| Smoking | 48 (11.1) | 26 (10.7) | 22 (11.6) | 0.772 | 20 (11.6) | 28 (10.7) | 0.770 |
| Obesity | 172 (39.7) | 97 (39.9) | 75 (39.5) | 0.925 | 66 (38.4) | 106 (40.6) | 0.641 |
| History of CAD | |||||||
| AMI | 22 (5.1) | 8 (3.3) | 15 (7.9) | 0.034 | 0 (0.0) | 22 (8.4) | <0.001 |
| PCI | 92 (21.2) | 40 (16.5) | 52 (27.4) | 0.006 | 6 (3.5) | 86 (33.0) | <0.001 |
| CABG | 18 (4.2) | 5 (2.1) | 13 (6.8) | 0.013 | 2 (1.2) | 16 (6.1) | 0.011 |
| Medication | |||||||
| Aspirin | 119 (27.5) | 51 (21.0) | 68 (35.8) | 0.001 | 16 (9.3) | 103 (39.5) | <0.001 |
| Oral anticoagulant | 19 (4.4) | 6 (2.5) | 13 (6.8) | 0.027 | 4 (2.3) | 15 (5.7) | 0.089 |
| TIMI score | 1.7 ± 1.3 | 1.4 ± 1.1 | 2.1 ± 1.3 | <0.001 | 0.9 ± 0.8 | 2.3 ±1.2 | <0.001 |
| GRACE score | 100.9 ± 26.1 | 94.7 ± 23.3 | 108.9 ± 27.3 | <0.001 | 85.8 ± 22.3 | 110.9 ± 23.4 | <0.001 |
| New ECG changes | 49 (11.3) | 16 (6.6) | 33 (17.4) | <0.001 | 11 (6.4) | 13 (14.6) | 0.009 |
Table 2.
Computed tomography coronary angiography findings stratified by troponin concentration and HEART score
| Variables | Overall (n=433) | hsTnI | HEART score | ||||
|---|---|---|---|---|---|---|---|
| <5 ng/L (n=243) | 5 ng/L to 99th percentile (n=190) | P-value | 0-3 (n=172) | ≥4 (n=261) | P-value | ||
| Stenosis | |||||||
| Normal | 112 (25.9) | 80 (32.9) | 32 (16.8) | <0.001 | 86 (50.0) | 26 (10.0) | <0.001 |
| Any CAD | 321 (74.1) | 163 (67.1) | 158 (83.2) | 86 (50.0) | 235 (90.0) | ||
| Normal or non-obstructive CAD | 313 (72.3) | 199 (81.9) | 114 (60.0) | <0.001 | 159 (92.4) | 154 (59.0) | <0.001 |
| Obstructive CAD | 120 (27.7) | 44 (18.1) | 76 (40.0) | 13 (7.6) | 107 (41.0) | ||
| Atherosclerotic burden | |||||||
| Segmental involvement score | 2 (0-5) | 2 (0-4) | 4 (1-6) | <0.001 | 1 (0-2) | 4 (2-6) | <0.001 |
| Calcium score | 15.4 (0-193.5) | 2.5 (0.0-99.3) | 91.5 (1.1-466.9) | <0.001 | 0.0 (0.0-12.0) | 112.1 (5.25-458.1) | <0.001 |
| Performance for detecting obstructive CAD, % (95% CI) | |||||||
| Sensitivity | 63.3 (54.1-71.9) | 89.2 (82.2-94.1) | |||||
| Specificity | 63.6 (58.0-68.9) | 50.8 (45.1-56.5) | |||||
| Positive predictive value | 40.0 (35.3-44.9) | 41.0 (37.9-44.1) | |||||
| Negative predictive value | 81.9 (77.9-85.3) | 92.4 (87.9-95.4) | |||||
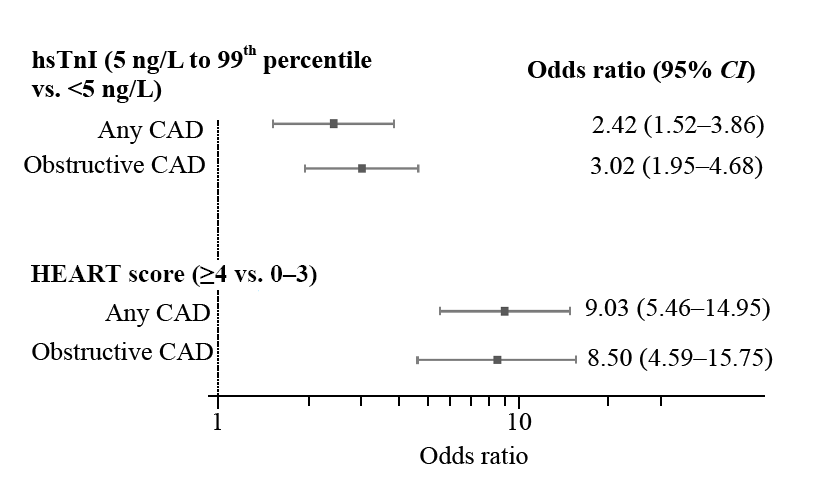
Figure 2.
Association between coronary artery disease and troponin concentration or HEART score. HEART: history, electrocardiography, age, risk factors, and troponin; CAD: coronary artery disease; CI: confidence interval.
| 1 | Fox WR, Diercks DB. Troponin assay use in the emergency department for management of patients with potential acute coronary syndrome: current use and future directions. Clin Exp Emerg Med. 2016; 3(1): 1-8. |
| 2 |
Kim MJ, Ha SO, Park YS, Yi JH, Yang WS, Kim JH. Validation and modification of HEART score components for patients with chest pain in the emergency department. Clin Exp Emerg Med. 2021; 8(4): 279-88.
doi: 10.15441/ceem.20.106 pmid: 35000355 |
| 3 |
Shin YS, Ahn S, Kim YJ, Ryoo SM, Sohn CH, Kim WY. External validation of the emergency department assessment of chest pain score accelerated diagnostic pathway (EDACS-ADP). Am J Emerg Med. 2020; 38(11): 2264-70.
doi: 10.1016/j.ajem.2019.09.019 pmid: 31757670 |
| 4 |
Shin YS, Ahn S, Kim YJ, Ryoo SM, Sohn CH, Seo DW, et al. Identifying low-risk chest pain in the emergency department: obstructive coronary artery disease and major adverse cardiac events. Am J Emerg Med. 2020; 38(9): 1737-42.
doi: S0735-6757(20)30501-5 pmid: 32738469 |
| 5 |
Keller T, Zeller T, Peetz D, Tzikas S, Roth A, Czyz E, et al. Sensitive troponin I assay in early diagnosis of acute myocardial infarction. N Engl J Med. 2009; 361(9): 868-77.
doi: 10.1056/NEJMoa0903515 |
| 6 |
Reichlin T, Hochholzer W, Bassetti S, Steuer S, Stelzig C, Hartwiger S, et al. Early diagnosis of myocardial infarction with sensitive cardiac troponin assays. N Engl J Med. 2009; 361(9): 858-67.
doi: 10.1056/NEJMoa0900428 |
| 7 |
Braunwald E, Morrow DA. Unstable angina: is it time for a requiem? Circulation. 2013; 127(24): 2452-7.
doi: 10.1161/CIRCULATIONAHA.113.001258 pmid: 23775194 |
| 8 |
Shah AS, Anand A, Sandoval Y, Lee KK, Smith SW, Adamson PD, et al. High-sensitivity cardiac troponin I at presentation in patients with suspected acute coronary syndrome: a cohort study. Lancet. 2015; 386(10012): 2481-8.
doi: 10.1016/S0140-6736(15)00391-8 pmid: 26454362 |
| 9 |
Chapman AR, Lee KK, McAllister DA, Cullen L, Greenslade JH, Parsonage W, et al. Association of high-sensitivity cardiac troponin I concentration with cardiac outcomes in patients with suspected acute coronary syndrome. JAMA. 2017; 318(19): 1913-24.
doi: 10.1001/jama.2017.17488 pmid: 29127948 |
| 10 |
Lee KK, Bularga A, O’Brien R, Ferry AV, Doudesis D, Fujisawa T, et al. Troponin-guided coronary computed tomographic angiography after exclusion of myocardial infarction. J Am Coll Cardiol. 2021; 78(14): 1407-17.
doi: 10.1016/j.jacc.2021.07.055 pmid: 34593122 |
| 11 |
Shin YS, Ahn S, Kim YJ, Ryoo SM, Sohn CH, Seo DW, et al. Modification of the HEART pathway by adding coronary computed tomography angiography for patients suspected of acute coronary syndrome in the emergency department. Intern Emerg Med. 2021; 16(2): 447-54.
doi: 10.1007/s11739-020-02419-8 |
| 12 |
Min JK, Shaw LJ, Devereux RB, Okin PM, Weinsaft JW, Russo DJ, et al. Prognostic value of multidetector coronary computed tomographic angiography for prediction of all-cause mortality. J Am Coll Cardiol. 2007; 50(12): 1161-70.
doi: 10.1016/j.jacc.2007.03.067 pmid: 17868808 |
| 13 |
Hoffmann U, Brady TJ, Muller J. Cardiology patient page. Use of new imaging techniques to screen for coronary artery disease. Circulation. 2003; 108(8): e50-3.
doi: 10.1161/01.CIR.0000085363.88377.F2 pmid: 12939244 |
| 14 |
DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988; 44(3): 837-45.
pmid: 3203132 |
| 15 |
Lambrakis K, Papendick C, French JK, Quinn S, Blyth A, Seshadri A, et al. Late outcomes of the rapid-TnT randomized controlled trial: 0/1-hour high-sensitivity troponin T protocol in suspected ACS. Circulation. 2021; 144(2):113-25.
doi: 10.1161/CIRCULATIONAHA.121.055009 pmid: 33998255 |
| 16 |
Six AJ, Backus BE, Kelder JC. Chest pain in the emergency room: value of the HEART score. Neth Heart J. 2008; 16(6): 191-6.
doi: 10.1007/BF03086144 pmid: 18665203 |
| 17 | Popa LE, Petresc B, Cătană C, Moldovanu CG, Feier DS, Lebovici A, et al. Association between cardiovascular risk factors and coronary artery disease assessed using CAD-RADS classification: a cross-sectional study in Romanian population. BMJ Open. 2020;10(1): e031799. |
| 18 |
Agewall S, Giannitsis E, Jernberg T, Katus H. Troponin elevation in coronary vs.non-coronary disease. Eur Heart J. 2011; 32(4): 404-11.
doi: 10.1093/eurheartj/ehq456 pmid: 21169615 |
| 19 |
Giannitsis E, Katus HA. Cardiac troponin level elevations not related to acute coronary syndromes. Nat Rev Cardiol. 2013; 10(11): 623-34.
doi: 10.1038/nrcardio.2013.129 pmid: 23979214 |
| 20 |
Sandoval Y, Bielinski SJ, Daniels LB, Blaha MJ, Michos ED, DeFilippis AP, et al. Atherosclerotic cardiovascular disease risk stratification based on measurements of troponin and coronary artery calcium. J Am Coll Cardiol. 2020; 76(4): 357-70.
doi: S0735-1097(20)35511-X pmid: 32703505 |
| 21 |
Neumann JT, Twerenbold R, Ojeda F, Sörensen NA, Chapman AR, Shah ASV, et al. Application of high-sensitivity troponin in suspected myocardial infarction. N Engl J Med. 2019; 380(26): 2529-40.
doi: 10.1056/NEJMoa1803377 |
| 22 |
Hamburger RF, Spertus JA, Winchester DE. Utility of the diamond-forrester classification in stratifying acute chest pain in an academic chest pain center. Crit Pathw Cardiol. 2016; 15(2): 56-9.
doi: 10.1097/HPC.0000000000000071 pmid: 27183255 |
| 23 |
Baskaran L, Danad I, Gransar H, Ó Hartaigh B, Schulman-Marcus J, Lin FY, et al. A comparison of the updated diamond-forrester, CAD consortium, and CONFIRM history-based risk scores for predicting obstructive coronary artery disease in patients with stable chest pain: the SCOT-HEART coronary CTA cohort. JACC Cardiovasc Imaging. 2019; 12(<W>7 pt 2):1392-400.
doi: 10.1016/j.jcmg.2018.02.020 |
| 24 |
Feger S, Ibes P, Napp AE, Lembcke A, Laule M, Dreger H, et al. Clinical pre-test probability for obstructive coronary artery disease: insights from the European DISCHARGE pilot study. Eur Radiol. 2021; 31(3): 1471-81.
doi: 10.1007/s00330-020-07175-z |
| 25 |
Wasfy MM, Brady TJ, Abbara S, Nasir K, Ghoshhajra BB, Truong QA, et al. Comparison of the diamond-forrester method and duke clinical score to predict obstructive coronary artery disease by computed tomographic angiography. Am J Cardiol. 2012; 109(7): 998-1004.
doi: 10.1016/j.amjcard.2011.11.028 pmid: 22236462 |
| [1] | Johan L. van Nieuwkerk, M. Christien van der Linden, Rolf J. Verheul, Merel van Loon-van Gaalen, Marije Janmaat, Naomi van der Linden. The impact of prehospital blood sampling on the emergency department process of patients with chest pain: a pragmatic non-randomized controlled trial [J]. World Journal of Emergency Medicine, 2023, 14(4): 257-264. |
| [2] | Jing-jing Xu, Si-da Jia, Lin Jiang, Ying Song, Pei Zhu, De-shan Yuan, Yi Yao, Xue-yan Zhao, Jian-xin Li, Yue-jin Yang, Shu-bin Qiao, Bo Xu, Run-lin Gao, Jin-qing Yuan. Prolonged dual antiplatelet therapy after drug-eluting stent implantation improves long-term prognosis for acute coronary syndrome: five-year results from a large cohort study [J]. World Journal of Emergency Medicine, 2023, 14(1): 25-30. |
| [3] | Guang-mei Wang, Yong Li, Shuo Wu, Wen Zheng, Jing-jing Ma, Feng Xu, Jia-qi Zheng, He Zhang, Jia-li Wang, Yu-guo Chen. The combination of creatine kinase-myocardial band isoenzyme and point-of-care cardiac troponin/ contemporary cardiac troponin for the early diagnosis of acute myocardial infarction [J]. World Journal of Emergency Medicine, 2022, 13(3): 163-168. |
| [4] | Li-wen Dou, Zhe Du, Ji-hong Zhu, Tian-bing Wang. Changes and significance of serum troponin in trauma patients: A retrospective study in a level I trauma center [J]. World Journal of Emergency Medicine, 2022, 13(1): 27-31. |
| [5] | Kun Cui, You-quan Shi, Yuan-zheng Zhang, Zheng-gong Li, Chang-ling Li. Optimized strategy of rotational atherectomy of underexpanded coronary stents in patients with acute coronary syndrome [J]. World Journal of Emergency Medicine, 2021, 12(3): 198-201. |
| [6] | Jing-jing Xu, Ying Song, Ping Jiang, Lin Jiang, Xue-yan Zhao, Zhan Gao, Jian-xin Li, Shu-bin Qiao, Run-lin Gao, Yue-jin Yang, Yin Zhang, Bo Xu, Jin-qing Yuan. Effects of metabolic syndrome on onset age and long-term outcomes in patients with acute coronary syndrome [J]. World Journal of Emergency Medicine, 2021, 12(1): 36-41. |
| [7] | Hai-mu Yao, Tong-wen Sun, You-dong Wan, Xiao-juan Zhang, Xin Fu, De-liang Shen, Jin-ying Zhang, Ling Li. Domestic versus imported drug-eluting stents for the treatment of patients with acute coronary syndrome [J]. World Journal of Emergency Medicine, 2014, 5(3): 175-181. |
| [8] | Li-ming Li, Wen-bo Cai, Qin Ye, Jian-min Liu, Xin Li, Xiao-xing Liao. Comparison of plasma microRNA-1 and cardiac troponin T in early diagnosis of patients with acute myocardial infarction [J]. World Journal of Emergency Medicine, 2014, 5(3): 182-186. |
| [9] | Lei Wang, Yi-tong Ma, Xiang Xie, Yi-ning Yang, Zhen-yan Fu, Fen Liu, Xiao-mei Li, Bang-dang Chen. Association of MMP-9 gene polymorphisms with acute coronary syndrome in the Uygur population of China [J]. World Journal of Emergency Medicine, 2011, 2(2): 104-110. |
| [10] | Shu-ming Pan, Chao-yang Tong, Qing Lin, Chen-ling Yao, Jie Zhao, Zhi Deng. Ischemia-modified albumin measured with ultra-filtration assay in early diagnosis of acute coronary syndrome [J]. World Journal of Emergency Medicine, 2010, 1(1): 37-40. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
