World Journal of Emergency Medicine ›› 2022, Vol. 13 ›› Issue (2): 114-119.doi: 10.5847/wjem.j.1920-8642.2022.027
• Original Articles • Previous Articles Next Articles
Hai Hu1,2( ), Jing-yuan Jiang2,3,4, Ni Yao2,3,4,5
), Jing-yuan Jiang2,3,4, Ni Yao2,3,4,5
Received:2021-08-29
Accepted:2021-11-20
Online:2021-12-31
Published:2022-03-01
Contact:
Hai Hu
E-mail:huhai@wchscu.cn
Hai Hu, Jing-yuan Jiang, Ni Yao. Comparison of different versions of the quick sequential organ failure assessment for predicting in-hospital mortality of sepsis patients: A retrospective observational study[J]. World Journal of Emergency Medicine, 2022, 13(2): 114-119.
Add to citation manager EndNote|Ris|BibTeX
URL: http://wjem.com.cn/EN/10.5847/wjem.j.1920-8642.2022.027
Figure 1.
Flow chart of case exclusions.
Table 1
Comparison of the baseline characteristics of survivors and non-survivors
| Variables | Survivors (n=835) | Non-survivors (n=101) | P value |
|---|---|---|---|
| Male | 509 (60.96) | 68 (67.33) | 0.234 |
| Age (years) | 50.13±18.32 | 58.91±20.92 | <0.001 |
| Temperature (°C) | 36.10±5.58 | 36.95±0.88 | 0.121 |
| Pulse (beats/min) | 105.46±69.60 | 103.27±24.76 | 0.753 |
| RR (breaths/min) | 21.62±5.96 | 22.74±5.49 | 0.072 |
| SBP (mmHg) | 113.19±37.60 | 107.18±36.63 | 0.129 |
| Mental status | |||
| Alert | 835 (100.0) | 51 (50.5) | <0.001 |
| Altered mentation | 0 (0.0) | 50 (49.5) | |
| SpO2 (%) | 95 (90-96) | 93 (89-94) | <0.001 |
| PCT (ng/mL) | 0.98 (0.66-5.91) | 1.23 (0.73-5.28) | 0.215 |
| Serum lactate (mmol/L) | 2.1 (1.7-2.8) | 2.5 (2.0-4.3) | <0.001 |
| SOFA | 4 (3-5) | 6 (5-8) | <0.001 |
| qSOFA | 1 (0-1) | 1 (1-2) | <0.001 |
| LqSOFA | 1 (0-2) | 2 (1-3) | <0.001 |
| PqSOFA | 1 (1-2) | 2 (1-3) | <0.001 |
| MqSOFA | 2 (1-2) | 3 (2-4) | <0.001 |
Table 2
The performance of scores with different cut-offs in predicting in-hospital mortality of sepsis patients
| Score | AUC | 95%CI | P value | Cut-off | Sen (%) | Spe (%) | PPV (%) | NPV (%) | Youden’s index |
|---|---|---|---|---|---|---|---|---|---|
| qSOFA | 0.705 | 0.645-0.764 | <0.001 | 1 | 80.20 | 42.16 | 14.36 | 94.62 | 0.224 |
| 2 | 39.60 | 91.62 | 36.36 | 92.62 | 0.312* | ||||
| 3 | 6.93 | 98.08 | 30.44 | 89.70 | 0.050 | ||||
| LqSOFA | 0.740 | 0.686-0.794 | <0.001 | 1 | 94.06 | 25.63 | 13.27 | 97.27 | 0.197 |
| 2 | 64.36 | 70.78 | 21.04 | 94.26 | 0.351* | ||||
| 3 | 28.71 | 95.57 | 43.94 | 91.72 | 0.243 | ||||
| 4 | 3.96 | 98.08 | 20.00 | 89.41 | 0.020 | ||||
| PqSOFA | 0.712 | 0.653-0.771 | <0.001 | 1 | 91.09 | 17.13 | 11.74 | 94.08 | 0.082 |
| 2 | 71.29 | 61.68 | 18.37 | 94.67 | 0.330* | ||||
| 3 | 31.68 | 93.89 | 38.55 | 91.91 | 0.256 | ||||
| 4 | 1.98 | 98.08 | 11.11 | 89.22 | 0.001 | ||||
| MqSOFA | 0.731 | 0.675-0.787 | <0.001 | 1 | 86.14 | 39.76 | 14.75 | 95.95 | 0.259 |
| 2 | 51.49 | 80.96 | 24.65 | 93.24 | 0.324* | ||||
| 3 | 25.74 | 97.01 | 50.98 | 91.53 | 0.227 | ||||
| 4 | 5.94 | 98.08 | 27.27 | 89.61 | 0.040 | ||||
| 5 | / | 98.08 | / | 89.02 | / |
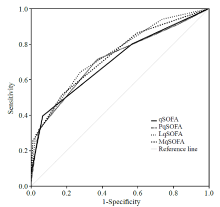
Figure 2.
ROC curves of different versions of the qSOFA in predicting in-hospital mortality. ROC: receiver operating characteristic; qSOFA: quick sequential organ failure assessment; LqSOFA: lactate-enhanced qSOFA; MqSOFA: modified qSOFA; PqSOFA: procalcitonin- enhanced qSOFA.
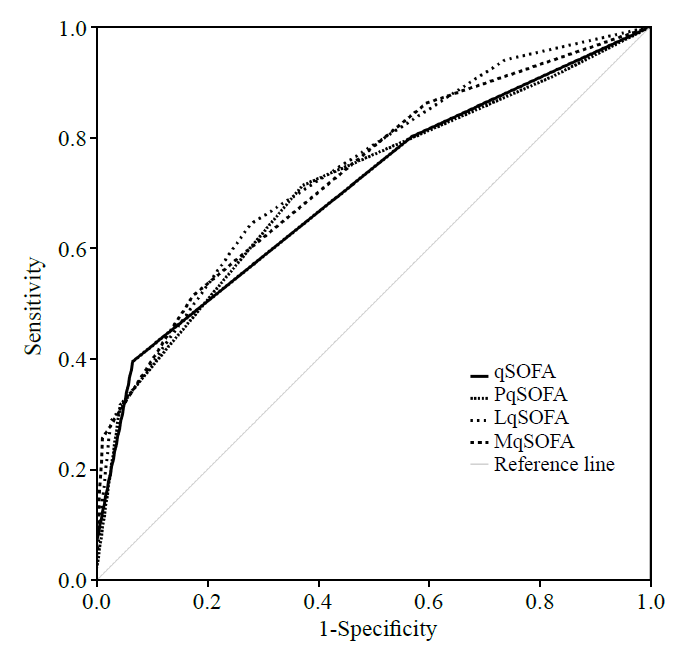
Table 3
Pairwise comparison of AUC of scores for predicting in-hospital mortality of sepsis patients
| Pairs of scores | ΔAUC | S.E. | 95%CI | P value |
|---|---|---|---|---|
| qSOFA vs. LqSOFA | 0.0353 | 0.0162 | 0.0035 to 0.0671 | 0.0295* |
| qSOFA vs. MqSOFA | 0.0266 | 0.0134 | 0.0003 to 0.0529 | 0.0478* |
| qSOFA vs. PqSOFA | 0.0072 | 0.0143 | -0.0208 to 0.0353 | 0.6129 |
| LqSOFA vs. MqSOFA | 0.0087 | 0.0178 | -0.0262 to 0.0436 | 0.6243 |
| LqSOFA vs. PqSOFA | 0.0281 | 0.0230 | -0.0170 to 0.0731 | 0.2218 |
| MqSOFA vs. PqSOFA | 0.0193 | 0.0201 | -0.0201 to 0.0588 | 0.3369 |
| 1 |
Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016; 315(8):801-10.
doi: 10.1001/jama.2016.0287 |
| 2 |
Vincent JL, Marshall JC, Namendys-Silva SA, François B, Martin-Loeches I, Lipman J, et al. Assessment of the worldwide burden of critical illness: the intensive care over nations (ICON) audit. Lancet Respir Med. 2014; 2(5):380-6.
doi: 10.1016/S2213-2600(14)70061-X |
| 3 |
Fleischmann C, Scherag A, Adhikari NK, Hartog CS, Tsaganos T, Schlattmann P, et al. Assessment of global incidence and mortality of hospital-treated sepsis. Current estimates and limitations. Am J Respir Crit Care Med. 2016; 193(3):259-72.
doi: 10.1164/rccm.201504-0781OC |
| 4 |
Iwashyna TJ, Ely EW, Smith DM, Langa KM. Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA. 2010; 304(16):1787-94.
doi: 10.1001/jama.2010.1553 |
| 5 |
Shu E, Ives Tallman C, Frye W, Boyajian JG, Farshidpour L, Young M, et al. Pre-hospital qSOFA as a predictor of sepsis and mortality. Am J Emerg Med. 2019; 37(7):1273-8.
doi: 10.1016/j.ajem.2018.09.025 |
| 6 |
Song JU, Sin CK, Park HK, Shim SR, Lee J. Performance of the quick sequential (sepsis-related) organ failure assessment score as a prognostic tool in infected patients outside the intensive care unit: a systematic review and meta-analysis. Crit Care. 2018; 22(1):28.
doi: 10.1186/s13054-018-1952-x |
| 7 |
Maitra S, Som A, Bhattacharjee S. Accuracy of quick sequential organ failure assessment (qSOFA) score and systemic inflammatory response syndrome (SIRS) criteria for predicting mortality in hospitalized patients with suspected infection: a meta-analysis of observational studies. Clin Microbiol Infect. 2018; 24(11):1123-9.
doi: 10.1016/j.cmi.2018.03.032 |
| 8 |
Liu YC, Luo YY, Zhang X, Shou ST, Gao YL, Lu B, et al. Quick sequential organ failure assessment as a prognostic factor for infected patients outside the intensive care unit: a systematic review and meta-analysis. Intern Emerg Med. 2019; 14(4):603-15.
doi: 10.1007/s11739-019-02036-0 |
| 9 |
Fernando SM, Tran A, Taljaard M, Cheng W, Rochwerg B, Seely AJE, et al. Prognostic accuracy of the quick sequential organ failure assessment for mortality in patients with suspected infection: a systematic review and meta-analysis. Ann Intern Med. 2018; 168(4):266-75.
doi: 10.7326/M17-2820 pmid: 29404582 |
| 10 |
Liu SJ, He CQ, He W, Jiang T. Lactate-enhanced-qSOFA (LqSOFA) score is superior to the other four rapid scoring tools in predicting in-hospital mortality rate of the sepsis patients. Ann Transl Med. 2020; 8(16):1013.
doi: 10.21037/atm |
| 11 |
Xia YQ, Zou LQ, Li DZ, Qin Q, Hu H, Zhou YW, et al. The ability of an improved qSOFA score to predict acute sepsis severity and prognosis among adult patients. Medicine (Baltimore). 2020; 99(5):e18942.
doi: 10.1097/MD.0000000000018942 |
| 12 |
Guarino M, Gambuti E, Alfano F, de Giorgi A, Maietti E, Strada A, et al. Predicting in-hospital mortality for sepsis: a comparison between qSOFA and modified qSOFA in a 2-year single-centre retrospective analysis. Eur J Clin Microbiol Infect Dis. 2021; 40(4):825-31.
doi: 10.1007/s10096-020-04086-1 |
| 13 | Hu H, Yao N, Qiu YR. Predictive value of 5 early warning scores for critical COVID-19 patients. Disaster Med Public Health Prep. 2020:1-8. |
| 14 |
DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988; 44(3):837-45.
pmid: 3203132 |
| 15 |
Waligora G, Gaddis G, Church A, Mills L. Rapid systematic review: the appropriate use of quick sequential organ failure assessment (qSOFA) in the emergency department. J Emerg Med. 2020; 59(6):977-83.
doi: 10.1016/j.jemermed.2020.06.043 |
| 16 |
Perman SM, Mikkelsen ME, Goyal M, Ginde A, Bhardwaj A, Drumheller B, et al. The sensitivity of qSOFA calculated at triage and during emergency department treatment to rapidly identify sepsis patients. Sci Rep. 2020; 10(1):20395.
doi: 10.1038/s41598-020-77438-8 pmid: 33230117 |
| 17 | Hwang SY, Jo IJ, Lee SU, Lee TR, Yoon H, Cha WC, et al. Low accuracy of positive qSOFA criteria for predicting 28-day mortality in critically ill septic patients during the early period after emergency department presentation. Ann Emerg Med. 2018; 71(1):1-9.e2. |
| 18 |
Moskowitz A, Patel PV, Grossestreuer AV, Chase M, Shapiro NI, Berg K, et al. Quick sequential organ failure assessment and systemic inflammatory response syndrome criteria as predictors of critical care intervention among patients with suspected infection. Crit Care Med. 2017; 45(11):1813-9.
doi: 10.1097/CCM.0000000000002622 pmid: 28759474 |
| 19 |
Askim Å, Moser F, Gustad LT, Stene H, Gundersen M, Åsvold BO, et al. Poor performance of quick-SOFA (qSOFA) score in predicting severe sepsis and mortality - a prospective study of patients admitted with infection to the emergency department. Scand J Trauma Resusc Emerg Med. 2017; 25(1):56.
doi: 10.1186/s13049-017-0399-4 |
| 20 |
Huson MA, Kalkman R, Grobusch MP, van der Poll T. Predictive value of the qSOFA score in patients with suspected infection in a resource limited setting in Gabon. Travel Med Infect Dis. 2017; 15:76-7.
doi: 10.1016/j.tmaid.2016.10.014 |
| 21 |
Donnelly JP, Safford MM, Shapiro NI, Baddley JW, Wang HE. Application of the Third International Consensus Definitions for Sepsis (Sepsis-3) Classification: a retrospective population-based cohort study. Lancet Infect Dis. 2017; 17(6):661-70.
doi: S1473-3099(17)30117-2 pmid: 28268067 |
| 22 |
Forward E, Konecny P, Burston J, Adhikari S, Doolan H, Jensen T. Predictive validity of the qSOFA criteria for sepsis in non-ICU inpatients. Intensive Care Med. 2017; 43(6):945-6.
doi: 10.1007/s00134-017-4776-2 pmid: 28357459 |
| 23 |
Oduncu AF, Kıyan GS, Yalçınlı S. Comparison of qSOFA, SIRS, and NEWS scoring systems for diagnosis, mortality, and morbidity of sepsis in emergency department. Am J Emerg Med. 2021; 48:54-9.
doi: 10.1016/j.ajem.2021.04.006 pmid: 33839632 |
| 24 |
Goulden R, Hoyle MC, Monis J, Railton D, Riley V, Martin P, et al. qSOFA, SIRS and NEWS for predicting inhospital mortality and ICU admission in emergency admissions treated as sepsis. Emerg Med J. 2018; 35(6):345-9.
doi: 10.1136/emermed-2017-207120 pmid: 29467173 |
| 25 |
Cecconi M, Evans L, Levy M, Rhodes A. Sepsis and septic shock. Lancet. 2018; 392(10141):75-87.
doi: 10.1016/S0140-6736(18)30696-2 |
| 26 |
Vincent JL, Quintairos E, Silva A, Couto L Jr, Taccone FS. The value of blood lactate kinetics in critically ill patients: a systematic review. Crit Care. 2016; 20(1):257.
doi: 10.1186/s13054-016-1403-5 |
| 27 | Khodashahi R, Sarjamee S. Early lactate area scores and serial blood lactate levels as prognostic markers for patients with septic shock: a systematic review. Infect Dis (Lond). 2020; 52(7):451-63. |
| 28 |
Baumann BM, Greenwood JC, Lewis K, Nuckton TJ, Darger B, Shofer FS, et al. Combining qSOFA criteria with initial lactate levels: Improved screening of septic patients for critical illness. Am J Emerg Med. 2020; 38(5):883-9.
doi: 10.1016/j.ajem.2019.07.003 |
| 29 |
Sinto R, Suwarto S, Lie KC, Harimurti K, Widodo D, Pohan HT. Prognostic accuracy of the quick Sequential Organ Failure Assessment (qSOFA)-lactate criteria for mortality in adults with suspected bacterial infection in the emergency department of a hospital with limited resources. Emerg Med J. 2020; 37(6):363-9.
doi: 10.1136/emermed-2018-208361 |
| 30 |
Leopold SJ, Ghose A, Plewes KA, Mazumder S, Pisani L, Kingston HWF, et al. Point-of-care lung ultrasound for the detection of pulmonary manifestations of malaria and sepsis: an observational study. PLoS One. 2018; 13(12):e0204832.
doi: 10.1371/journal.pone.0204832 |
| 31 | Rice TW, Wheeler AP, Bernard GR, Hayden DL, Schoenfeld DA, Ware LB, et al. Comparison of the SpO2/FiO2 ratio and the PaO2/FiO2 ratio in patients with acute lung injury or ARDS. Chest. 2007; 132(2):410-7. |
| 32 |
Pepper DJ, Sun JF, Rhee C, Welsh J, Powers JH 3rd, Danner RL, et al. Procalcitonin-guided antibiotic discontinuation and mortality in critically ill adults: a systematic review and meta-analysis. Chest. 2019; 155(6):1109-18.
doi: 10.1016/j.chest.2018.12.029 |
| 33 | Robati Anaraki M, Nouri-Vaskeh M, Abdoli Oskouie S. Effectiveness of procalcitonin-guided antibiotic therapy to shorten treatment duration in critically-ill patients with bloodstream infections: a systematic review and meta-analysis. Infez Med. 2020; 28(1):37-46. |
| 34 |
Liu D, Su LX, Han GC, Yan P, Xie LX. Prognostic value of procalcitonin in adult patients with sepsis: a systematic review and meta-analysis. PLoS One. 2015; 10(6):e0129450.
doi: 10.1371/journal.pone.0129450 |
| 35 |
AlRawahi AN, AlHinai FA, Doig CJ, Ball CG, Dixon E, Xiao ZW, et al. The prognostic value of serum procalcitonin measurements in critically injured patients: a systematic review. Crit Care. 2019; 23:390.
doi: 10.1186/s13054-019-2669-1 |
| [1] | Li-wei Duan, Jin-long Qu, Jian Wan, Yong-hua Xu, Yi Shan, Li-xue Wu, Jin-hao Zheng, Wei-wei Jiang, Qi-tong Chen, Yan Zhu, Jian Zhou, Wen-bo Yu, Lei Pei, Xi Song, Wen-fang Li, Zhao-fen Lin. Effects of viral infection and microbial diversity on patients with sepsis: A retrospective study based on metagenomic next-generation sequencing [J]. World Journal of Emergency Medicine, 2021, 12(1): 29-35. |
| [2] | Hai-jiang Zhou, Tian-fei Lan, Shu-bin Guo. Outcome prediction value of National Early Warning Score in septic patients with community-acquired pneumonia in emergency department: A single-center retrospective cohort study [J]. World Journal of Emergency Medicine, 2020, 11(4): 206-215. |
| [3] | Yu-ming Wang, Yan-jun Zheng, Ying Chen, Yun-chuan Huang, Wei-wei Chen, Ran Ji, Li-li Xu, Zhi-tao Yang, Hui-qiu Sheng, Hong-ping Qu, En-qiang Mao, Er-zhen Chen. Effects of fluid balance on prognosis of acute respiratory distress syndrome patients secondary to sepsis [J]. World Journal of Emergency Medicine, 2020, 11(4): 216-222. |
| [4] | Miao Yuan, Ding-yi Yan, Fang-shi Xu, Yi-di Zhao, Yang Zhou, Long-fei Pan. Effects of sepsis on hippocampal volume and memory function [J]. World Journal of Emergency Medicine, 2020, 11(4): 223-230. |
| [5] | Wen-peng Yin, Jia-bao Li, Xiao-fang Zheng, Le An, Huan Shao, Chun-sheng Li. Effect of neutrophil CD64 for diagnosing sepsis in emergency department [J]. World Journal of Emergency Medicine, 2020, 11(2): 79-86. |
| [6] | Shao-hua Liu, Huo-yan Liang, Hong-yi Li, Xian-fei Ding, Tong-wen Sun, Jing Wang. Effect of low high-density lipoprotein levels on mortality of septic patients: A systematic review and meta-analysis of cohort studies [J]. World Journal of Emergency Medicine, 2020, 11(2): 109-116. |
| [7] | Yi-wen Fan, Shao-wei Jiang, Jia-meng Chen, Hui-qi Wang, Dan Liu, Shu-ming Pan, Cheng-jin Gao. A pulmonary source of infection in patients with sepsis-associated acute kidney injury leads to a worse outcome and poor recovery of kidney function [J]. World Journal of Emergency Medicine, 2020, 11(1): 18-26. |
| [8] | Kimberly A. Chambers, Adam Y. Park, Rosa C. Banuelos, Bryan F. Darger, Bindu H. Akkanti, Annamaria Macaluso, Manoj Thangam, Pratik B. Doshi. Outcomes of severe sepsis and septic shock patients after stratification by initial lactate value [J]. World Journal of Emergency Medicine, 2018, 9(2): 113-117. |
| [9] | Muhammad Akbar Baig, Hira Shahzad, Erfan Hussain, Asad Mian. Validating a point of care lactate meter in adult patients with sepsis presenting to the emergency department of a tertiary care hospital of a low- to middle-income country [J]. World Journal of Emergency Medicine, 2017, 8(3): 184-189. |
| [10] | Chao Cao, Tao Ma, Yan-fen Chai, Song-tao Shou. The role of regulatory T cells in immune dysfunction during sepsis [J]. World Journal of Emergency Medicine, 2015, 6(1): 5-9. |
| [11] | Kun Chen, Qiu-xiang Zhou, Hong-wei Shan, Wen-fang Li, Zhao-fen Lin. Prognostic value of CD4+CD25+ Tregs as a valuable biomarker for patients with sepsis in ICU [J]. World Journal of Emergency Medicine, 2015, 6(1): 40-43. |
| [12] | Hui Fu, Qiao-sheng Wang, Qiong Luo, Si Tan, Hua Su, Shi-lin Tang, Zheng-liang Zhao, Li-ping Huang. Simvastatin inhibits apoptosis of endothelial cells induced by sepsis through upregulating the expression of Bcl-2 and downregulating Bax [J]. World Journal of Emergency Medicine, 2014, 5(4): 291-297. |
| [13] | Qi Zou, Wei Wen, Xin-chao Zhang. Presepsin as a novel sepsis biomarker [J]. World Journal of Emergency Medicine, 2014, 5(1): 16-19. |
| [14] | Nishant Raj Pandey, Yu-yao Bian, Song-tao Shou. Significance of blood pressure variability in patients with sepsis [J]. World Journal of Emergency Medicine, 2014, 5(1): 42-47. |
| [15] | Huan Ding, Xiang-yuan Cao, Xi-gang Ma, Wen-jie Zhou. Endothelial cell injury with inflammatory cytokine and coagulation in patients with sepsis [J]. World Journal of Emergency Medicine, 2013, 4(4): 285-289. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
