World Journal of Emergency Medicine ›› 2020, Vol. 11 ›› Issue (1): 37-47.doi: 10.5847/wjem.j.1920-8642.2020.01.006
Special Issue: Poisoning
• Original Articles • Previous Articles Next Articles
Shi-yuan Yu1, Yan-xia Gao2, Joseph Walline3, Xin Lu1, Li-na Zhao1, Yuan-xu Huang4, Jiang Tao4, An-yong Yu5, Na Ta6, Ren-ju Xiao7, Yi Li1( )
)
Received:2019-02-20
Accepted:2019-09-08
Online:2020-01-01
Published:2020-01-01
Contact:
Yi Li
E-mail:billliyi@126.com
Shi-yuan Yu, Yan-xia Gao, Joseph Walline, Xin Lu, Li-na Zhao, Yuan-xu Huang, Jiang Tao, An-yong Yu, Na Ta, Ren-ju Xiao, Yi Li. Role of penehyclidine in acute organophosphorus pesticide poisoning[J]. World Journal of Emergency Medicine, 2020, 11(1): 37-47.
Add to citation manager EndNote|Ris|BibTeX
URL: http://wjem.com.cn//EN/10.5847/wjem.j.1920-8642.2020.01.006
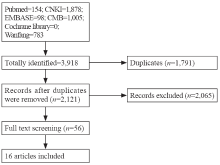
Figure 1.
Flow diagram.

Table 1
Included articles
| First author | Journal | Organophosphate component | N | Drug administration |
|---|---|---|---|---|
| Lin et al[ | Chinese Journal of Modern Drug Application | Not reported | 150 | Penehyclidine+atropine group, atropine 10-20 mg IV and penehyclidine 1 mg IM three times a day, then atropine 5-10 mg every 5-10 minutes until atropinization; penehyclidine group, penehyclidine 4-6 mg IM then penehyclidine 2-3 mg every 1-2 hours until atropinization; atropine group, atropine 10-20 mg IV then 5-10 mg IV every 5-10 minutes until atropinization |
| Wu et al[ | Heilongjiang Medical Journal | Not reported | 83 | Penehyclidine group, penehyclidine 4-6 mg IV initially; atropine group, atropine 10-20 mg IV initially |
| Fu et al[ | 11th National Conference on Disaster Medicine with Integrated Traditional Chinese Medicine and Western Medicine | Not reported | 62 | Penehyclidine group, penehyclidine 4-6 mg IM initially then 1-2 mg until atropinization; atropine group, atropine 20-40 mg IV initially |
| Zhao et al[ | World Notes | Not reported | 48 | Penehyclidine+atropine group, penehyclidine 4-6 mg IM initially, atropine 1-2 mg every 8-12 hours; atropine group, atropine 10-20 mg IM every 1 hour until atropinization |
| Liang et al[ | Contemporary Medicine | Not reported | 120 | Penehyclidine+atropine group, atropine 10-20 mg IV initially then 5-10 mg every 5-10 minutes until atropinization, then Penehyclidine 1-2 mg IM every 8-12 hours; atropine group, atropine 10-20 mg IV initially then 5-10 mg every 5-10 minutes until atropinization |
| Sun et al[ | China Modern Medicine | Not reported | 58 | Penehyclidine+atropine group, penehyclidine 4-5 mg IM+atropine 10-20 mg IV initially; atropine group, atropine 10-20 mg IV then additional atropine every 10-30 minutes until atropinization |
| Zeng et al[ | Fujian Medicine Journal | Not reported | 62 | Penehyclidine group, penehyclidine 4-6 mg IM initially; atropine group, atropine 3-5 mg IV then 5-15 mg every 5-10 minutes until atropinization |
| Liu et al[ | Medical Innovation of China | Dichlorvos, omethoate, rogor, methamidophos, dipterex | 64 | Penehyclidine group, penehyclidine 5 mg IV, then 3 mg every 30-60 minutes until atropinization; atropine group, atropine 10 mg IV initially |
| Chen et al[ | Guide of China Medicine | Cynamid, alkron, demeton, methamidophos, rogor | 80 | Penehyclidine+atropine group, penehyclidine 1 mg IM+atropine 10-20 mg IV, then atropine 10 mg every 10-15 minutes until atropinization |
| Guan et al[ | World Latest Medicine Information | Not reported | 60 | Penehyclidine+atropine group, penehyclidine 4-6 mg IM initially, then atropine IV until atropinization; atropine group, atropine 10-15 mg IV every 10-30 minutes until atropinization |
| Wang et al[ | Chinese Journal of Modern Drug Application | Cynamid, alkron, methamidophos, dichlorvos, rogor, azodrin, phoxime | 76 | Penehyclidine+atropin group, penehyclidine 2-3 mg IM +atropine 5-10 mg IV, then 5-10 mg atropine every 5-10 minutes until atropinization; penehyclidine group, 4 mg IM, additional drug due to patients condition until atropinization; atropine group, 5-10 mg atropine IV, then 5-10 mg atropine every 5-10 minutes until atropinization |
| Yi et al[ | Journal of Lingnan Emergency Medicine | Dichlorvos, methamidophos, acephate, alkron, malathion | 102 | Penehyclidine+atropin group, atropine 10 mg intravenously (IV) + penehyclidine 5 mg intramuscularly (IM), then 5 mg atropine every 5-10 minutes until atropinization; penehyclidine group, 6 mg penehyclidine IM then 3 mg penehyclidine IM every 30 minutes until atropinization; atropine group, 10 mg atropine IV then 5 mg atropine IV until atropinization |
| Luo et al[ | Medicine | Methamidophos, dichlorvos, rogor, dipterex | 98 | Penehyclidine+atropine group, atropine 10-15 mg IV and penehyclidine 4-6 mg IM, then atropine IV until atropinization; penehyclidine group, penehyclidine 4-6 mg IM initially; atropine group, atropine 10-15 mg IV every 10-30 minutes until atropinization |
| Shi et al[ | Journal of Clinical Emergency | Omethoate, dichlorvos, methamidophos | 56 | Penehyclidine group, penehyclidine 6 mg IV, then 3 mg every 30-60 minutes until atropinization; atropine group, atropine 20 mg IV initially |
| Zhou et al[ | Occupation and Health | Dichlorvos, alkron, rogor, methamidophos, cynamid, demeton | 180 | Penehyclidine+atropine group, penehyclidine 4-6 mg IM+atropine 3-5 mg IV, then atropine 3-5 mg atropine every 3-5 minutes until atropinization; penehyclidine group, penehyclidine 4-6 mg IM, then 2-3 mg after 30-60 minutes, then 1-2 mg until atropinization; atropine group, atropine 5-10 mg IV, then 5-10 mg every 5-10 minutes until atropinization |
| Liu et al[ | Modern Journal of Integrated Traditional Chinese and Western Medicine | Not reported | 35 | Penehyclidine group, penehyclidine 4-6 mg IM initially; atropine group, atropine 10-20 mg IV then 5-15 mg every 15-30 minutes until atropinization |
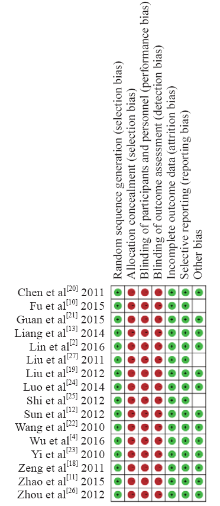
Figure 2.
Risk of bias summary.
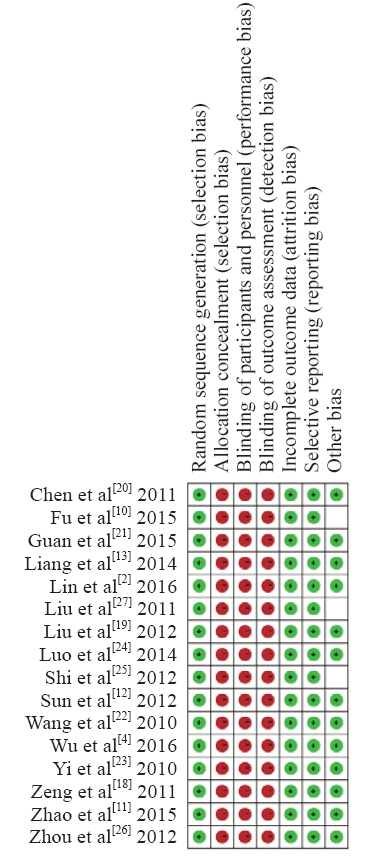

Figure 3.
Cured rate.

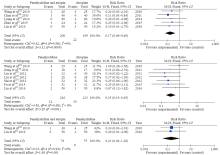
Figure 4.
Mortality rate.
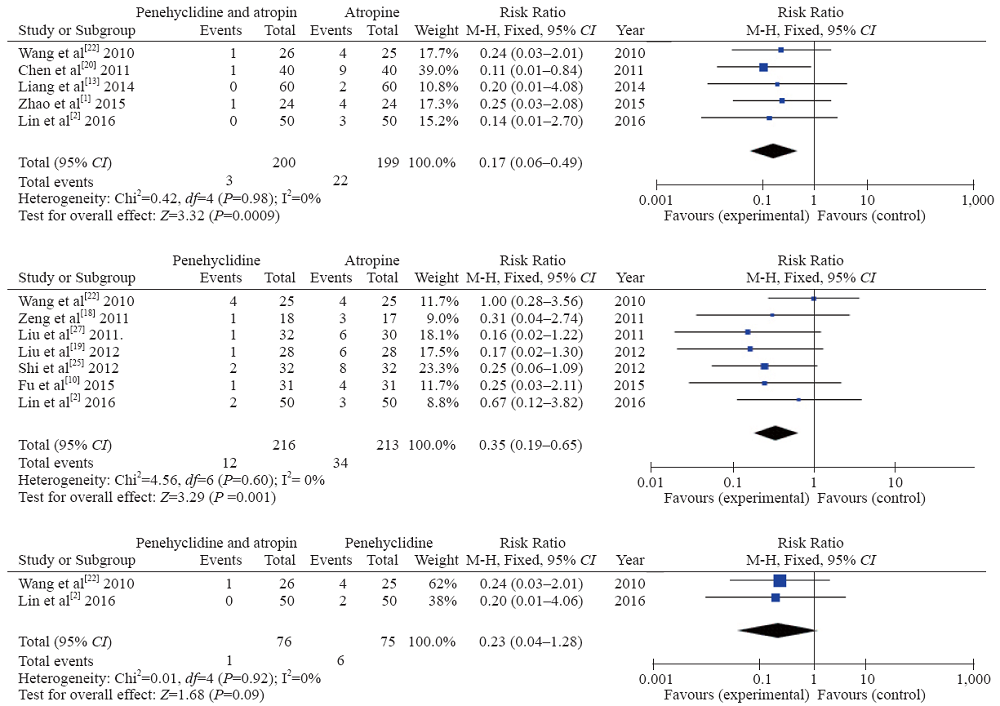
Table 2
Main outcomes
| Variables | Penehyclidine and atropine vs. Atropine | Penehyclidine vs. Atropine | Penehyclidine and atropine vs. Penehyclidine | ||||||
|---|---|---|---|---|---|---|---|---|---|
| RR or SMD | 95% CI | P | RR or SMD | 95% CI | P | RR or SMD | 95% CI | P | |
| Cured rate | 1.13 | 1.07-1.19 | <0.00001 | 1.16 | 1.08-1.24 | <0.00001 | 1.08 | 1.01-1.15 | 0.02 |
| Mortality rate | 0.17 | 0.06-0.49 | 0.0009 | 0.35 | 0.19-0.65 | 0.001 | 0.23 | 0.04-1.28 | 0.09 |
| Time to atropinization | -1.44 | -2.37- -0.51 | 0.002 | 1.00 | 0.75-1.26 | <0.00001 | -1.53 | -1.53- -1.24 | <0.00001 |
| Time of AchE back to 60% | -1.69 | -1.89- -1.48 | <0.00001 | -1.27 | -1.53- -1.01 | <0.00001 | -0.77 | -1.83-0.30 | 0.16 |
| Rate of IMS | 0.31 | 0.15-0.64 | 0.002 | 0.39 | 0.21-0.70 | 0.002 | 0.70 | 0.28-1.78 | 0.45 |
| Rate of total ADR | 0.19 | 0.09-0.41 | <0.00001 | - | - | - | - | - | - |
| Time of hospitalization | -1.35 | -1.74- -0.95 | <0.00001 | -0.42 | -0.85-0.01 | 0.06 | -1.40 | -3.64-0.84 | 0.22 |
| 1 |
Perera PM, Jayamanna SF, Hettiarachchi R, Abeysinghe C, Karunatilake H, Dawson AH, et al. A phase II clinical trial to assess the safety of clonidine in acute organophosphorus pesticide poisoning. Trials. 2009; 10:73.
doi: 10.1186/1745-6215-10-73 pmid: 19691854 |
| 2 | Lin TL. Atropine, penehyclidine hydrochloride combined with blood perfusion on severe organophosphorus poisoning patients. Chin J Mod Drug Appl. 2016; 10(12):156-7. |
| 3 | Chen W, Huang ML, Wei SC. Rate of delirium between Penehyclidine and atropine therapy on acute organophosphorus poisoning. Chin J Mod Med. 2016; 2(11):68-71. |
| 4 | Wu HK. Clinical observation of penehyclidine hydrochloride treating 42 cases of severe acute organophosphorus patients. Heilongjiang Med J. 2016; 40(10):928-29. |
| 5 | Li M. Consensus on diagnosis and management of acute poisoning. Chinese Journal of Hygiene Rescue (Electronic Edition). 2016; 12(6):333-47. |
| 6 | Ai L. Administration of combined anticholinergic agents on acute organophophours poisoning patients. Journal of Nursing. 2015; 2(5):91-3. |
| 7 |
Katz FS, Pecic S, Schneider L, Zhu Z, Hastings A, Luzac M, et al. New therapeutic approaches and novel alternatives for organophosphate toxicity. Toxicol Lett. 2018; 291:1-10.
pmid: 29614332 |
| 8 |
Brvar M, Chan MY, Dawson AH, Ribchester RR, Eddleston M. Magnesium sulfate and calcium channel blocking drugs as antidotes for acute organophosphorus insecticide poisoning - a systematic review and meta-analysis. Clin Toxicol (Phila). 2018; 56(8):725-36.
doi: 10.1080/15563650.2018.1446532 |
| 9 |
Dawson AH, Buckley NA. Pharmacological management of anticholinergic delirium - theory, evidence and practice. Br J Clin Pharmacol. 2016; 81(3):516-24.
pmid: 26589572 |
| 10 | Fu SZ, Yang LY, Tan Y, Dong H. Comparison between penehyclidine and atropine on rescuing severe acute organophosphorus poisoning patients. 11th National Conference on Disaster Medicine with Integrated Traditional Chinese Medicine and Western Medicine. P2. |
| 11 | Zhao JS. Clinical analysis of penehyclidine hydrochloride injection combined with atropine in the treatment of acute severe organophophorus pesticide poisoning. World Notes on Antibiotics. 2015; 36(4):191-2. |
| 12 | Guo Y, Wei M, Yan Z, Wang G. Penehyclidine hydrochloride attenuates LPS-induced acute lung injury in rats. Molecular Medicine Journal. 2017; 33(11):1486-90. |
| 13 | Liang CK, He SF, Li WS. Clinical analysis of Penehyclidine combined with atropine in the resuscitation procedure of acute severe organophophorus poisoning. Contemporary Medicine. 2014; 20(19):86-7. |
| 14 | Sun LS. Clinical outcomes and prognosis of penehyclidine hydrochloride combined with atropine on treating acute organophosphorus pesticide poisoning patients. Chian Modern Medicine. 2012; 19(21):102-4. |
| 15 | Li CM. Study of management on severe acute organophosphorus pesticide poisoning. China Pharmacology. 2015; 20(17):95-6. |
| 16 |
Sun L, Li GQ, Yan PB, Liu Y, Li GF, Wei LQ. Clinical management of organophosphate poisoning in pregnancy. Am J Emerg Med. 2015; 33(2):305.e1-3.
doi: 10.1016/j.ajem.2014.05.057 |
| 17 | Chen JY, Duan B, Liu JY. Outcomes of penehyclidine hydrochloride and atropine in treating acute organophosphorus pesticide poisoning: A meta-analysis. Clinical Misdiagnosis & Mistherapy. 2012; 7(5):71-4. |
| 18 | Zeng P, Lei LH, Wang WP. Clinical observation of Penehyclidine treating severe organophosphorus poisoning and analysis of 62 cases. Fujian Medical Journal. 2011; 33(4):126-7. |
| 19 | Liu YB, Huang YH, Chen XZ, Zeng MH. Comparison between penehyclidine and atropine of outcomes on resuscitation procedure of acute severe organophosphorus poisoning. Medical Innovation of China. 2012; 9(14):46-7. |
| 20 | Chen BX. Outcomes of penehyclidine combined with atropine on treating severe acute organophosphorus poisoning. Guide of China Medicine. 2011; 15(9):225-6. |
| 21 | Guan HY. Outcomes of penehyclidine combined with atropine in treating severe organophosphorus poisnoing. World Latest Medicine Information. 2015; 15(53):62. |
| 22 | Wang LX. Outcomes of penehyclidine combined with atropine on treating severe organophosphorus pesticide poisoning. Chin J Mod Drug Appl. 2010; 11(4):121-2. |
| 23 | Yi F, Lu HH, Wang Y, Peng K, Chen P, Tang B. Clinical observation of penehyclidine combined with atropine on treating severe organophosphorus pesticide poisoning. Journal of Lingnan Emergency Medicine. 2010; 15(2):133-5. |
| 24 | Luo SH. Clinical outcomes of Penehyclidine combined with atropine on treating severe organophosphorus pesticide poisoning. Medicine. 2014; 8(9):415-6. |
| 25 | Shi J. Application of penehyclidine hydrochloride in severe organophosphorus poisoning. Journal of Clinical Emergency Call (China). 2012; 13(2):132-3. |
| 26 | Zhou JW, Xue Y, Zhang RG, Yao L, Tian ZY, Du GJ. Clinical observation of penehyclidine hydrochloride combined with atropine in the treatment of acute severe organophosphorus poisoning. Occupation and Health. 2012; 28(15):1918-20. |
| 27 | Liu M, Liang XG. Clinical outcomes of penehyclidine hydrochloride in rescuing severe organophosphorus poisoning. Modern Journal of Integrated Traditional Chinese and Western Medicine. 2011; 20(30):3816-7. |
| 28 | Xue F. Outcomes of Penehyclidine combined with atropine in treating acute severe organophosphorus pesticide poisoning patients. Chinese Folk Medicine. 2010; 12(7):180-9. |
| 29 |
Mew EJ, Padmanathan P, Konradsen F, Eddleston M, Chang SS, Phillips MR, et al. The global burden of fatal self-poisoning with pesticides 2006-15: Systematic review. J Affect Disord. 2017; 219:93-104.
doi: 10.1016/j.jad.2017.05.002 pmid: 28535450 |
| 30 |
Moffatt A, Mohammed F, Eddleston M, Azher S, Eyer P, Buckley NA. Hypothermia and fever after organophosphorus poisoning in humans--a prospective case series. J Med Toxicol. 2010; 6(4):379-85.
doi: 10.1007/s13181-010-0012-y pmid: 20300985 |
| 31 |
Jayasinghe SS, Pathirana KD, Buckley NA. Effects of acute organophosphorus poisoning on function of peripheral nerves: a cohort study. PLoS One. 2012; 7(11):e49405.
doi: 10.1371/journal.pone.0049405 pmid: 23185328 |
| 32 |
Yuan QH, Xiao F, Liu QS, Zheng F, Shen SW, He QW, et al. M 3 receptor is involved in the effect of penehyclidine hydrochloride reduced endothelial injury in LPS-stimulated human pulmonary microvascular endothelial cell. Pulm Pharmacol Ther. 2018; 48(2):144-50.
doi: 10.1016/j.pupt.2017.11.007 |
| 33 |
Yu C, Wang J. Neuroprotective effect of penehyclidine hydrochloride on focal cerebral ischemia-reperfusion injury. Neural Regen Res. 2013; 8(7):622-32.
doi: 10.3969/j.issn.1673-5374.2013.07.006 pmid: 25206707 |
| 34 |
Shu Y, Yang Y, Zhang P. Neuroprotective effects of penehyclidine hydrochloride against cerebral ischemia/reperfusion injury in mice. Brain Res Bull. 2016; 121:115-23.
doi: 10.1016/j.brainresbull.2016.01.008 pmid: 26802510 |
| 35 |
Wang J, Ren Y, Zhu Y, Chen JW, Zhu MM, Xu YJ, et al. Effect of penehyclidine hydrochloride on the incidence of intra-operative awareness in Chinese patients undergoing breast cancer surgery during general anaesthesia. Anaesthesia. 2013; 68(2):136-41.
doi: 10.1111/anae.12092 |
| 36 |
Cao HJ, Sun YJ, Zhang TZ, Zhou J, Diao YG. Penehyclidine hydrochloride attenuates the cerebral injury in a rat model of cardiopulmonary bypass. Can J Physiol Pharmacol. 2013; 91(7):521-7.
doi: 10.1139/cjpp-2012-0329 pmid: 23827043 |
| 37 |
Pandit JJ, Picton P, Mashour GA. Penehcyclidine and awareness during anaesthesia: caution with zero numerators. Anaesthesia. 2013; 68(2):131-5.
pmid: 23237632 |
| 38 |
Wang YP, Li G, Ma LL, Zheng Y, Zhang SD, Zhang HX, et al. Penehyclidine hydrochloride ameliorates renal ischemia-reperfusion injury in rats. J Surg Res. 2014; 186(1):390-7.
doi: 10.1016/j.jss.2013.07.041 pmid: 23972620 |
| 39 |
Xiao HT, Liao Z, Tong RS. Penehyclidine hydrochloride: a potential drug for treating COPD by attenuating Toll-like receptors. Drug Des Devel Ther. 2012; 6:317-22.
doi: 10.2147/DDDT.S36555 pmid: 23139625 |
| 40 |
Shadnia S, Zamani N, Hassanian-Moghaddam H, Shafaroodi H, Padandar M, Rezaeizadeh MH. Prognostic value of cortisol and thyroid function tests in poisoned patients admitted to toxicology ICU. World J Emerg Med. 2018; 9(1):51-5.
doi: 10.5847/wjem.j.1920-8642.2018.01.008 pmid: 29290896 |
| 41 |
Eddleston M, Dawson A, Karalliedde L, Dissanayake W, Hittarage A, Azher S, et al. Early management after self-poisoning with an organophosphorus or carbamate pesticide - a treatment protocol for junior doctors. Crit Care. 2004; 8(6):R391-7.
doi: 10.1186/cc2953 pmid: 15566582 |
| 42 |
Wang W, Chen QF, Li QB, Wu YB, Chen K, Chen B, et al. Efficiency of anisodamine for organophosphorus-poisoned patients when atropinization cannot be achieved with high doses of atropine. Environ Toxicol Pharmacol. 2014; 37(2):477-81.
doi: 10.1016/j.etap.2013.12.016 pmid: 24561530 |
| [1] | Yu-qing Cui, Xian-fei Ding, Huo-yan Liang, Dong Wang, Xiao-juan Zhang, Li-feng Li, Quan-cheng Kan, Le-xin Wang, Tong-wen Sun. Efficacy and safety of low-dose corticosteroids for acute respiratory distress syndrome: A systematic review and meta-analysis [J]. World Journal of Emergency Medicine, 2021, 12(3): 207-213. |
| [2] | Xin Lu, Wei Han, Yan-xia Gao, Shi-gong Guo, Shi-yuan Yu, Xue-zhong Yu, Hua-dong Zhu, Yi Li. Efficacy and safety of corticosteroids in immunocompetent patients with septic shock [J]. World Journal of Emergency Medicine, 2021, 12(2): 124-130. |
| [3] | Shao-hua Liu, Huo-yan Liang, Hong-yi Li, Xian-fei Ding, Tong-wen Sun, Jing Wang. Effect of low high-density lipoprotein levels on mortality of septic patients: A systematic review and meta-analysis of cohort studies [J]. World Journal of Emergency Medicine, 2020, 11(2): 109-116. |
| [4] | Gan-nan Wang, Xu-feng Chen, Li Qiao, Yong Mei, Jin-ru Lv, Xi-hua Huang, Bin Shen, Jin-song Zhang. Comparison of extracorporeal and conventional cardiopulmonary resuscitation: A meta-analysis of 2 260 patients with cardiac arrest [J]. World Journal of Emergency Medicine, 2017, 8(1): 5-11. |
| [5] | Li-ping Chen, Jun-hui Chen, Ying Chen, Chao Wu, Xiao-hong Yang. Efficacy and safety of glucocorticoids in the treatment of community-acquired pneumonia: A meta-analysis of randomized controlled trials [J]. World Journal of Emergency Medicine, 2015, 6(3): 172-178. |
| [6] | Mohsen Ebrahimi, Abbas Heydari, Reza Mazlom, Amir Mirhaghi. The reliability of the Australasian Triage Scale: a meta-analysis [J]. World Journal of Emergency Medicine, 2015, 6(2): 94-99. |
| [7] | Xu-rui Luo, Hui-li Zhang, Geng-jin Chen, Wen-shu Ding, Liang Huang. Active compression-decompression cardiopulmonary resuscitation (CPR) versus standard CPR for cardiac arrest patients: a meta-analysis [J]. World Journal of Emergency Medicine, 2013, 4(4): 266-272. |
| [8] | Xiao-ping Wang, Qing-ming Lin, Shen Zhao, Shi-rong Lin, Feng Chen. Therapeutic benefits of mild hypothermia in patients successfully resuscitated from cardiac arrest:A meta-analysis [J]. World Journal of Emergency Medicine, 2013, 4(4): 260-265. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
