World Journal of Emergency Medicine ›› 2016, Vol. 7 ›› Issue (1): 5-12.doi: 10.5847/wjem.j.1920-8642.2016.01.001
• Review Article • Next Articles
Alaaddin M Salih1,2( ), Musab Alfaki3, Dafalla M Alam-Elhuda4
), Musab Alfaki3, Dafalla M Alam-Elhuda4
Received:2015-09-20
Accepted:2016-01-12
Online:2016-03-15
Published:2016-03-15
Contact:
Alaaddin M Salih
E-mail:alaaddinsalih@yahoo.com
Alaaddin M Salih, Musab Alfaki, Dafalla M Alam-Elhuda. Airway foreign bodies: A critical review for a common pediatric emergency[J]. World Journal of Emergency Medicine, 2016, 7(1): 5-12.
Add to citation manager EndNote|Ris|BibTeX
URL: http://wjem.com.cn//EN/10.5847/wjem.j.1920-8642.2016.01.001
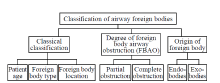
Figure 1.
Classification of airway foreign bodies.


Figure 2.
AFB emergency algorithm following ERC and AHA guidelines. ERC: European Resuscitation Council; AHA: American Heart Association; FB: foreign bodies; CPR: cardiopulmonary resuscitation; ERS: emergency response system.

| 1 | Limper AH, Prakash UB. Tracheobronchial foreign bodies in adults. Ann Intern Med 1990; 112:604-609. |
| 2 | Haugen RK. The café coronary: sudden deaths in restaurants. JAMA 1963; 186:142-143. |
| 3 | Fleischer K. Erkennung und Entfernung Von. Bronchial-frem-dkorpern-einstJetzt. TherGgegenw 1974; 113:348-358. |
| 4 | Robinson CLN, Mushin WW. Inhaled foreign bodies. Br Med J 1956; 2:324-328. |
| 5 | El-Munshid HA. Gastrointestinal Physiology. In: Sukkar MY, El-Munshid HA, Ardawi MSM. Concise Human Physiology. 2nd Ed. Oxford: Blackwell; 2000; 159. |
| 6 | Park JY, Elshami AA, Kang DS, Jung TH. Plastic bronchitis. Eur Respir J 1996; 9:612-614. |
| 7 | Passàli D, Lauriello M, Bellussi L, Passali GC, Passali FM, Gregori D. Foreign body inhalation in children: an update. Acta Otorhinolaryngol Ital 2010; 30:27-32. |
| 8 |
Hughes CA, Baroody FM, Marsh BR. Pediatric tracheobronchial foreign bodies: Historical review from the Johns Hopkins Hospital. Ann Otol Rhinol Laryngol 1996; 105:555-561.
pmid: 8678434 |
| 9 | Centres for Disease Control and Prevention (CDC). Nonfatal choking-related episodes among children-United States, 2002; 51:945. |
| 10 | Doody DP. Foreign body aspiration. In: Grillo HC. Surgery of the Trachea and Bronchi. 1st Ed. Ontario: BC Decker Inc.; 2004; 707-718. |
| 11 |
Ciftci AO, Bingöl-Koloğlu M, Senocak ME, Tanyel FC, Büyükpamukçu N. Bronchoscopy for evaluation of foreign body aspiration in children. J Pediatr Surg; 38:1170-1176.
pmid: 12891487 |
| 12 | Reilly JS, Cook SP, Stool D, Rider G. Prevention and management of aerodigestive foreign body injuries in childhood. Pediatr Clin North Am 1996; 43:1403-1411. |
| 13 |
Smith GA, Gardner HG, Baum CR, Dowd MD, Durbin DR, Lichenstein R, et al. Prevention of chocking among children. Pediatrics 2010; 125:601-607.
pmid: 20176668 |
| 14 | Yadav SP, Singh J, Aggarwal N, Goel A. Airway foreign bodies in children: experience of 132 cases. Singapo Med J 2007; 48:850-853. |
| 15 | Brkić F, Umihanić S. Tracheobronchial foreign bodies in children. Experience at ORL clinic Tuzla, 1954-2004. Int J Pediatr Otorhinolaryngol 2007; 71:909-915. |
| 16 | Shivakumar AM, Naik AS, Prashanth KB, Shetty KD, Praveen DS. Tracheobronchial foreign bodies. Indian J Pediatr 2003; 70:793-797. |
| 17 |
Chiu CY, Wong KS, Lai SH, Hsia SH, Wu CT. Factors predicting early diagnosis of foreign body aspiration in children. Pediatr Emerg Care 2005; 21:161-164.
pmid: 15744193 |
| 18 |
Cohen SR, Herbert WI, Lewis GB Jr, Geller KA. Foreign bodies in the airway - 6 year retrospective study with special reference to management. Ann Otol Rhinol Laryngol 1980; 89:437-442.
pmid: 7436248 |
| 19 | Kaur K, Sonkhya N, Bapna AS. Foreign bodies in the tracheobronchial tree: a prospective study of fifty cases. Indi J Otolaryngol Head Nec Surg 2002; 54:30-34. |
| 20 | Hughes C, Anthony E. Paediatric tracheobronchial foreign bodies - historical review from the John Hopkins Hospital. Ann Otol Rhinol Laryngol 1996; 105:555-561. |
| 21 |
Shlizerman L, Ashkenazi D, Mazzawi S, Harefuah RY. Foreign body aspiration in children: ten-years experience at the Ha'Emek Medical Center. Harefuah 2006; 145:569-571, 631.
pmid: 16983838 |
| 22 |
Foltran F, Ballali S, Rodriguez H, Bvan A, Desiderio A, Desiderio P, et al. Inhaled foreign bodies in children: a global perspective on their epidemiological, clinical, and preventive aspects. Pediatr Pulmonol 2013; 48:344-351.
pmid: 23169545 |
| 23 |
Baharloo F, Veyckemans F, Francis C, Biettlot MP, Rodenstein DO. Tracheobronchial foreign bodies: presentation and management in children and adults. Chest 1999; 115:1357-1362.
doi: 10.1378/chest.115.5.1357 pmid: 10334153 |
| 24 |
Lan RS. Non asphyxiating tracheobronchial foreign bodies in adults. Eur Respir J 1994; 7:510-514.
pmid: 8013610 |
| 25 | Patel S, Kazeroonl EA. Case 31: foreign body aspiration-chicken vertebra. Radiol 2001; 218:523-525. |
| 26 | Vijayasekaran D, Sambandam AP, Gowrishankar NC. Acute plastic bronchitis. Indian Paediatr 2004 Dec 17; 41:1257-1259. |
| 27 |
Ragab A, Ebied OM, Zalat S. Scarf pins sharp metallic tracheobronchial foreign bodies: presentation and management. Int J Pediatr Otorhinolaryngol 2007; 71:769-773.
doi: 10.1016/j.ijporl.2007.01.018 pmid: 17343924 |
| 28 | Review of inhaled foregin body. Amsterdam: Elsevier Inc.; 24 Aug 2007. http://www.mdconsult.com/. |
| 29 | Alfageme I, Reyes N, Merino M. Aspirated foreign body. Int J Pulmon Med 2007; 7:5-6. |
| 30 |
Webb WA. Management of foreign bodies of the upper gastrointestinal tract. Gastrointest Endosc 1995; 41:39-51.
pmid: 7698623 |
| 31 | Ganong WF. Review of Medical Physiology. 22th Ed. London: McGraw-Hill; 2005; 678. |
| 32 | Inhaled foregin body. Florida: DSHI Systems Inc.; 27 Apr 2009. Available from: http://www.freemd.com/. |
| 33 | Poirier M. Foreign bodies of the respiratory tract. Intern J Emerg Med 2003; 2:1-12. |
| 34 |
Brownstein D, Hodge D. Foreign bodies of the eye, ear, and nose. Pediatr Emerg Care 1988; 4:215-218.
doi: 10.1097/00006565-198809000-00016 pmid: 3186530 |
| 35 |
Baker M. Foreign bodies of the ears and nose in childhood. Pediatr Emerg Care 1987; 3:67-70.
doi: 10.1097/00006565-198706000-00001 pmid: 3615236 |
| 36 |
Bennett J. An unexplained cause of halitosis. J R Army Med Corps 1988; 134:151-152.
pmid: 3193395 |
| 37 | Fireman P. Diagnosis of sinusitis in children: emphasis on the history and physical examination. J A Clin Immunol 1992; 90:433-436. |
| 38 | Jackson C, Jackson CL. Diseases of the Air and Food Passages of Foreign Body Origin. 1st Ed. Philadelphia, PA: Elsevier Saunders; 1936. |
| 39 | Mehta S, Mehta N, Suri M, Khajura R. Guidelines for removal of foreign bodies in pediatric airway. JK Practiti 2006; 13:18-22. |
| 40 |
Denny MK, Berkas EM, Snider TH. Foreign body bronchiectasis. Dis Chest 1968; 53:613-616.
doi: 10.1378/chest.53.5.613 pmid: 5658975 |
| 41 |
Pinzoni F, Boniotti C, Molinaro SM, Baraldi A, Berlucchi M. Inhaled foreign bodies in pediatric patients: review of personal experience. Int J Pediatr Otorhinolaryngol 2007; 71:1897-1903.
doi: 10.1016/j.ijporl.2007.09.002 |
| 42 |
Pinto A, Scaglione M, Pinto F, Guidi G, Pepe M, Del Prato B, Grassi R, et al. Tracheobronchial aspiration of foreign bodies: current indications for emergency plain chest radiography. Radiol Med 2006; 111:497-506.
doi: 10.1007/s11547-006-0045-0 pmid: 16779536 |
| 43 | Chew HS, Kiaang Tan HK. Airway foreign body in children. Int J Clin Med 2012; 3:655-660. |
| 44 |
Hoeve LJ, Rombout J, Pot DJ. Foreign body aspiration in children. The diagnostic value of signs, symptoms and preoperative examination. Clin Otolaryngol 1993; 18:55-57.
pmid: 8448893 |
| 45 |
Fontoba JEB, Gutierrez C, Lluna J, Vila JJ, Poquet J, Ruiz-Company S. Bronchial foreign body: should bronchoscopy be performed in all patients with a chocking crisis? Pediatr Surg Int 1997; 12:118-120.
pmid: 9156835 |
| 46 | Merghani TH. The core of medical physiology. 1st Ed. Khartoum: Khartoum University Printing Press; 2008. |
| 47 | Agarwal RK, Banerjee G, Shembish N, Jamal B, Kareemullah C, Swaleh ABV. Foreign bodies in the tracheobronchial tree: a review of 102 cases in Benghazi, Libya. Ann Trop Pediatr 1988; 8:213-216. |
| 48 |
Singh B, Kantu M, Har-El G, Lucente FE. Complications associated with 327 foregin bodies of the pharynx, larynx, &esophagus. Ann Otol Rhinol Laryngol 1997; 106:301-304.
pmid: 9109720 |
| 49 | Sapira JD, Orient JM. Sapira's art & science of bedside diagnosis. Hagerstwon: Lippincott Williams & Wilkins; 2000. |
| 50 |
Zerellaab JT, Dimlerab M, McGillab LC, Pippus KJ. Foreign body aspiration in children: Value of radiography and complications of bronchoscopy. J Pediatr Surg 1998; 33:1651-1654.
doi: 10.1016/s0022-3468(98)90601-7 pmid: 9856887 |
| 51 |
Ginsberg GG. Management of ingested foreign objects & food bolus impactions. Gastrointest Endosc, 1995; 41:33-38.
doi: 10.1016/S0016-5107(95)70273-3 pmid: 7698622 |
| 52 |
Hoeve LJ, Rombout J, Pot DJ. Foreign body aspiration in children: The diagnostic value of signs, symptoms and pre-operative examination. Clin Otolaryngo & Allie Scien 1993; 18:55-57.
doi: 10.1111/coa.1993.18.issue-1 |
| 53 |
Heyer CM, Bollmeier ME, Rossler L, Nuesslein TG, Stephan V, Bauer TT, et al. Evaluation of clinical, radiologic, and laboratory prebronchoscopy findings in children with suspected foreign body aspiration. J Pediatr Surg 2006; 41:1882-1888.
pmid: 17101364 |
| 54 |
Kadmon G, Stern Y, Bron-Harlev E, Nahum E, Battat E, Schonfeld T. Computerized scoring system for the diagnosis of foreign body aspiration in children. Ann Otol Rhinol Laryngol 2008; 117:839-843.
doi: 10.1177/000348940811701108 pmid: 19102130 |
| 55 | Cantaneo AJ, Reibscheid SM, Ruiz Junior RL, Ferrari GF. Foreign body in the tracheobronchial tree. Clin Pediatr 1997; 36:701-706. |
| 56 | Loo CM, Hsu AAL, Eng P, Ong YY. Case series of bronchoscopic removal of tracheobronchial foreign body in six adults. Ann Acad Med Singapore 1998; 27:849-853. |
| 57 | Svedstrom E, Puhakka H, Kero P. How accurate is chest radiography in the diagnosis of tracheobronchial foreign bodies in children?. Pediatr Radiol 1989; 19:521-522. |
| 58 | Griffiths DM, Freeman NV. Expiratory chest X-ray examination in the diagnosis of inhaled foreign bodies. Br Med J 1984; 288:1074-1075. |
| 59 | Assefa D, Amin N, Stringel G, Dozor AJ. Use of Decubitus radiographs in the diagnosis of foreign body aspiration in young children. Pediatr Emerg Care Mar 2007; 23:154-157. |
| 60 |
Virk J, Pang J, Okhovat S, Lingam R, Singh A. Analysis lateral soft tissue neck radiographs. Emerg Radiol 2012; 19:255-260.
pmid: 22351123 |
| 61 |
Even L, Heno N, Talmon Y, Samet E, Zonis Z, Kugelman A. Diagnostic evaluation of foreign body aspiration in children: a prospective study. J Pediatr Surg 2005; 40:1122-1127.
pmid: 16034756 |
| 62 |
Hong SJ, Goo HW, Roh JL. Utility of Spiral and cine CT scans in pediatric patients suspected of aspirating radiolucent foreign bodies. Otolaryngol Head Neck Surg 2008; 138:576-580.
doi: 10.1016/j.otohns.2007.12.039 pmid: 18439461 |
| 63 | Donnellyl F, Frush DP, Risset GS, The multiple presentations of foreign bodies in children. Am J Roentgenol 1998; 170:471-477. |
| 64 |
Tokar B, Ozkan R, Ilhan H. Tracheobronchial foreign bodies in children: importance of accurate history and plain chest radiography in delayed presentation. Clin Radiol 2004; 59:609-615.
pmid: 15208067 |
| 65 |
Hagan JF, Shaw JS, Duncan PM, editors. Bright Future: Guidelines for Health Supervision of Infants, Children, and Adolescents. 3rd Ed. Elk Grove Village, IL: American Academy of Pediatrics; 2008.
pmid: 11581444 |
| 66 | Biarent D, Bingham R, Eich C, López-Herce J, Maconochie I, Rodríguez-Núñez A, et al. European Resuscitation Council Guidelines for Resuscitation 2010: Section 6, Paediatric life support. Resuscita 2010; 31:1364-88. |
| 67 |
Berg MD, Schexnayder SM, Chameides L, Terry M, Donoghue A, Hickey RW, et al. Part 13: Pediatric Basic Life Support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2010; 122:S862-S875.
doi: 10.1161/CIRCULATIONAHA.110.971085 pmid: 20956229 |
| 68 |
Swanson KL, Prakash UBS, Midthun DE, Edell ES, Utz JP, McDougall JC, et al. Flexible Bronchoscopic Management of Airway Foreign Bodies in Children. Chest 2003; 121:1695-700.
pmid: 12006464 |
| 69 | Swanson KL, Parkash USB, McDougall JC. Airway foreign bodies in adults. J Bronchol 2003; 10:107-111. |
| 70 | Surka A, Chin R, Conforti J. Bronchoscopic myths and legends: airway foreign bodies. Clin Pulm Med 2006; 3:209-211. |
| 71 |
Ramírez-Figueroa JL, Gochicoa-Rangel LG, Ramírez-San Juan DH, Vargas MH. Foreign body removal by flexible fiberoptic bronchoscopy in infants and children. Pediatr Pulmonol 2005; 40:392-397.
doi: 10.1002/ppul.20242 pmid: 16130115 |
| 72 |
Tang LF, Xu YC, Wang YS, Wang CF, Zhu GH, Bao XE, et al. Airway foreign body removal by flexible bronchoscopy: experience with 1027 children during 2000-2008. World J Pediatr 2009; 5:191-195.
pmid: 19693462 |
| 73 |
Sepehr A, Albers GC, Armstrong WB. Aspiration of a capsule endoscope and description of a unique retrieval technique. Otolaryngol Head Neck Surg 2007; 137:965-966.
doi: 10.1016/j.otohns.2007.09.011 pmid: 18036432 |
| 74 | Steen KH, Zimmermann T. Tracheobronchial aspiration of foreign bodies in children: a study of 94 cases. Laryngoscop 1990; 100:925-930. |
| 75 |
Elhassani NB. Tracheobronchial foreign bodies in the Middle East: A Baghdad study. J Thorac Cardiovasc Surg 1988; 96:621-625.
pmid: 3172808 |
| 76 |
Hsu Wc, Sheen Ts, Lin Cd, Tan Ct, Yeh Th, Lee Sy. Clinical experiences of removing foreign bodies in the airway and esophagus with a rigid endoscope: a seies of 3217 cases from 1970 to 1996. Otolaryngol Head Neck Surg 2000; 122:450-454.
doi: 10.1067/mhn.2000.98321 pmid: 10699826 |
| 77 |
Solanki SL, Bansal S, Khare A, Jain A. Heimlich's maneuver-assisted bronchoscopic removal of airway foreign body. Anesth Essays Res 2011; 5:201-203.
pmid: 25885389 |
| 78 |
Ulku R, Onen A, Onat S, Ozcelik C. The value of surgical approaches for aspirated pen caps. J Pediatr Surg 2005; 40:1780-1783.
pmid: 16291169 |
| 79 |
Zhijun C, Fugao Z, Niankai Z, Jingjing C. Therapeutic experience from 1420 patients with pediatric tracheobronchial foreign body. J Pediatr Surg 2008; 43:718-721.
doi: 10.1016/j.jpedsurg.2007.10.010 pmid: 18405721 |
| 80 | Weir PM. Foreign body aspiration. In: Stoddart PA, Lauder GR, editors. Problems in Anaesthesia: Paediatric Anaesthesia. 1st Ed. London: Taylor & Francis Books Ltd.; 2004; 163-166. |
| 81 | Soodan A, Pawar D, Subramanium R. Anaesthesia for removal of inhaled foreign bodies in children. Pediatr Anaesth 2004; 14:947-952. |
| 82 | Hidaka H, Obara T, Kuriyama S, Kurosawa S, Katori Y, Kobayashi T. Logistic regression analysis of risk factors for prolonged pulmonary recovery in children from aspirated foreign body. Int J Pediat Otorhinolaryngol 2013; 77:1677-1682. |
| 83 |
Williams A, George C, Atul PS, Sam S, Shukla S. An audit of morbidity and mortality associated with foreign body aspiration in children from a tertiary level hospital in Northern India. Afr J Paediatr Surg 2014; 11:287-292.
pmid: 25323175 |
| 84 | Foreign body aspiration-Diagnosis-Best Practice [homepage on the Internet]. London: BMJ Publishing Group; 2010. Available from: http://www.bestpractice.bmj.com/. |
| 85 | MacSween RNM, Whaley K. Muir's Textbook of Pathology. 13th Ed. London: Arnold; 1992. |
| 86 | Oliveira CF, Almeida JFL, Troster EJ, Costa Vaz FA. Complications of tracheobronchial foreign body aspiration in children: report of 5 cases and review of the literature. Rev Hosp Clin 2002; 57:108-111. |
| 87 |
de Sousa ST, Ribeiro VS, de Menezes Filho JM, dos Santos AM, Barbieri MA, de Figueiredo Neto JA. Foreign body aspiration in children and adolescents: experience of a Brazilian referral center. J Bras Pneumol 2009; 35:653-659.
doi: 10.1590/S1806-37132009000700006 pmid: 19669003 |
| 88 |
Rodríguez H, Cuestas G, Botto H, Nieto M, Cocciaglia A, Passali D, et al. Complications in children from foreign bodies in the airway. Acta Otorrinolaringol Esp 2015 Apr 6; pii: S0001-6519(15)00031-X. doi: 10.1016/j.otorri.2015.01.003.
doi: 10.1016/j.otorri.2020.04.009 pmid: 32862972 |
| 89 |
Kaur K, Sonkhya N, Bapna AS. Foreign bodies in the tracheobronchial tree: A prospective study of fifty cases. Indian J Otolaryngol Head Neck Surg 2002; 54:30-34.
pmid: 23119848 |
| 90 |
Fidkowski CW, Zheng H, Firth PG. The anesthetic considerations of tracheobronchial foreign bodies in children: A literature review of 12 979 cases. Anesth Analg 2010; 111:1016-1025.
pmid: 20802055 |
| 91 | Foltran F, Ballali S, Passali FM, Kern E, Morra B, Passali GC, et al. Foreign bodies in the airways: A meta-analysis of published papers. Int J Pediatr Otorhinolaryngol 2012; 76S:S12-S19. |
| 92 |
Sane SM, Faerber EN, Belani KK. Respiratory foreign bodies and Eikenella corrodens brain abscess in two children. Pediatr Radiol 1999; 29:327-330.
pmid: 10382208 |
| 93 |
Roberts J, Bartlett AH, Giannoni CM, Valdez TA. Airway foreign bodies and brain abscesses: report of two cases and review of the literature. Int J Pediatr Otorhinolaryngol 2008; 72:265-269.
pmid: 18031834 |
| 94 |
Tuggey JM, Hosker HSR, DaCosta P. Primary pulmonary botryomycosis: a late complication of foreign body aspiration. Thorax 2000; 55:1068-1069.
pmid: 11083895 |
| [1] | Liliana Costa, Ricardo Matos, Sara Júlio, Fernando Vales, Margarida Santos. Urgent tracheostomy: four-year experience in a tertiary hospital [J]. World Journal of Emergency Medicine, 2016, 7(3): 227-230. |
| [2] | Derinoz Oksan, Belen F. Burcu, Yılmaz Sebahat. Is tracheostomy suitable for securing airway after facial firearm injuries? [J]. World Journal of Emergency Medicine, 2011, 2(4): 307-309. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
