


Trans-anal barotrauma resulting from the use of air guns is rare in the emergency department. Early diagnosis and timely treatment can yield a good prognosis. The first published case of trans-anal barotrauma caused by a manually operated force pump was reported in 1904.[1] Colorectal injuries have the potential to progress to high-mortality complications, such as abdominal infection, peritonitis, and septic shock.[2,3] Herein, we report a case of trans-anal barotrauma in a man who presented with pneumoperitoneum, pneumomediastinum, and pneumoscrotum. We performed laparoscopic exploration and loop ileostomy on this patient.
In July 2023, a 25-year-old young man presented to our emergency department 9 h after being shot by his playmates through the anus with an air gun during a play session. He complained of abdominal distension and anus pain, with a Numerical Rating Scale (NRS) score of 3-4. On general examination, the patient was conscious, with a blood pressure of 117/52 mmHg (1 mmHg=0.133 kPa) and a heart rate of 79 beats/min. On physical examination, there was deep tenderness on the right side of the abdomen without rebound tenderness. Subcutaneous crepitation was observed in the chest and abdomen. The scrotum and penis were obviously swollen. A digital rectal examination was unable to be performed because of pain in the anus.
A computed tomography (CT) scan revealed pneumatosis in the mediastinum around the heart and aorta and pneumatosis in the abdomen around the anus, rectum and sigmoid colon. Gas was also found to accumulate at the perineum, scrotum, pelvis, retroperitoneal space, and colon wall of the rectum and sigmoid colon (Figure 1). Ultrasonography of the urinary system revealed gas around the right kidney, which was also observed on the CT scan. The results of laboratory tests, including arterial blood gas, complete blood count, liver and kidney function, and coagulation tests, were unremarkable.
Figure 1.
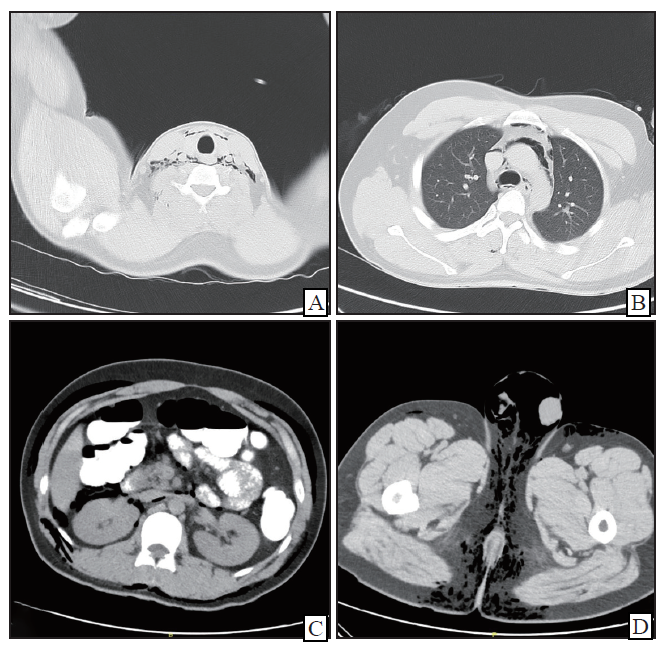
Figure 1.
Computed tomography of the patient. A: pneumatosis in the neck; B: pneumatosis beside the aorta; C: pneumatosis around the right kidney; D: pneumatosis at the scrotum.
This patient was diagnosed with trans-anal barotrauma. An emergency laparoscopic exploration was performed, but no apparent perforation was found. The degree of abdominal contamination was mild. To prevent occult colonic perforation, ileostomy was performed. The operation took 60 min, and the volume of blood lost was approximately 20 mL.
During the whole treatment process, we closely monitored the patient’s respiratory and circulatory conditions. The patient was successfully extubated on the 1st day after the operation and returned to the general ward from the ICU. The CT scan was performed again on the 3rd day after the operation, which revealed that the mediastinal emphysema had been absorbed. Meropenem was given for anti-infection treatment. His body temperature returned to normal on the 5th day after the operation, his white blood cell count decreased to 9.35×109/L, and his C-reactive protein level decreased to 33.60 mg/L. The patient was discharged on the 7th day after changing to oral antibiotics. After two months, the patient underwent ileostomy closure and had no sequelae.
Trans-anal barotrauma is rare in the emergency department, and its diagnosis and treatment pose certain difficulties. We carefully reviewed published cases of trans-anal barotrauma from the PubMed database. The detailed outcomes and demographics of each patient are reported in supplementary Table 1. Most trans-anal barotrauma patients are injured due to jokes or pranks from their friends.[4] This highlights the need for strict training and education for high-pressure air equipment users.
Colorectal injuries are usually observed following motor vehicle accidents or invasive therapeutic procedures such as colonoscopy or barium enema.[5] The most common cause of colon barotrauma is iatrogenic injury from colonoscopy, with an incidence of 3.1-12.0 per 10,000 procedures.[6⇓-8] Barotrauma can directly cause intestinal perforation and abdominal organ rupture.[9⇓-11] When high-pressure air enters the intestines, the serosal layer would first tear, followed by the mucosa and muscle. According to a previous experimental study, intestine perforation occurred at pressures ranging from 0.49 to 0.88 kg/cm2 in dogs. The required average pressure was 0.29 kg/cm2 for human gastrointestinal tract perforation completely.[12]
In our patient, no obvious colon perforation was found during the operation. However, the observation of contamination within the abdomen suggested the possibility of occult perforation. Among the reviewed patients, 30 patients had confirmed perforations, 1 patient was suspected of occult perforation, and only 1 patient showed no sign of perforation and then received conservative treatment.
The perforation location was mainly in the rectum and rectosigmoid junction for most patients, which was associated with the gas pressure distribution in the intestines. The ileocecal valve prevents gas from entering the small intestine. High-pressure air within the colon creates a gas pressure gradient from the anus to the ileocecal valve. Therefore, most trans-anal barotrauma patients experience perforations in the distal colon and rectum.
The complications of trans-anal barotrauma include peritonitis, sepsis, hemorrhagic shock, pneumoperitoneum, and pneumomediastinum.[13,14] Intestinal canal perforation may lead to pneumoperitoneum. Intestinal content leakage may cause abdominal infection and sepsis. Organ rupture can induce hemorrhagic shock. The air can also enter the mediastinum through subcutaneous emphysema to form pneumomediastinum. The continuous entry of air leads to increased abdominal pressure and may affect other organs’ blood supplements, which may ultimately cause circulatory failure. Emergency doctors should be aware that colorectal injuries have the potential to be highly fatal.
In our literature review, only one case has been reported using laparoscopic technology to treat trans-anal barotrauma,[15] while the other patients underwent exploratory laparotomy. The underlying reason may be that the tiny incisions used in laparoscopic surgery could hinder the handling of unforeseen circumstances during emergency procedures. With the increasing proportion of laparoscopic surgeries in emergency procedures in recent years,[16,17] the advantages of laparoscopic surgery in emergency surgeries have gradually been confirmed, including faster postoperative recovery, minimal trauma, and fewer postoperative complications.[18,19] Fortunately, we performed laparoscopic exploration and loop ileostomy on this patient and succeeded without any sequelae.
Among the 35 patients we reviewed, only 4 died, 1 of whom died before arriving at the hospital. With proper assignment and timely treatment and the development of prehospital emergency care, the prehospital mortality of trans-anal barotrauma caused by high-pressure air has a very good prognosis.
Owing to the one-way valve function of the ileocecal valve, intestinal perforations from rectal pressure injuries always occur in the colon. We recommend that surgeons choose a prophylactic ileostomy instead of a transverse colostomy for highly suspected perforation patients, which benefits undetected occult colonic perforations.
In conclusion, trans-anal barotrauma induced by high-pressure air is mainly caused by pranks and jokes. This condition may be life-threatening without prompt treatment. Owing to the barrier effect of the ileocecal valve, most perforations occur within the colon, and the perforation site is likely located near the anus. Timely exploration is crucial for trans-anal barotrauma patients, and prophylactic ileotomy is recommended for occult perforations.
Funding: This research was supported by National High Level Hospital Clinical Research Funding (2022-PUMCH-B-110).
Ethical approval: This study was approved by the Medical Ethics Committee of Peking Union Medical College Hospital, and the participants provided written informed consent.
Conflicts of interest: The authors have no conflicts of interest to declare.
Contributors: JX and HDZ designed the entire study and provided critical clinical advice. CXL and LZ contributed to the data collection, analysis and interpretation and were major contributors to the writing of the manuscript. All the authors read and approved the final manuscript.
All the supplementary files in this paper are available at http://wjem.com.cn.
Reference
A case of rupture of the bowel caused by compressed air
Prophylactic antibiotics for penetrating abdominal trauma
Management of perforated diverticulitis with generalized peritonitis. A multidisciplinary review and position paper
Rupture of sigmoid colon caused by compressed air
Colorectal barotrauma following compressed air spray to the perineum
Adverse events related to colonoscopy: global trends and future challenges
Screening for colorectal cancer: updated evidence report and systematic review for the US preventive services task force
Colonoscopic perforations: a review of 30,366 patients
Pneumatic colon injury following high pressure blow gun dust cleaner spray to the perineum
Rectal perforation by compressed air
A case of pneumatic rectal perforation caused by compressed air
Trans-anal barotrauma by compressed air leading to sigmoid perforation due to a dangerous practical joke
Fatal air pressure injuries of the intestine: a case report
Colon perforation by compressed air: a case report and short review of literature
Emergency laparoscopic resection of the anterior rectum due to rectal trauma secondary to compressed air, case report
Sepsis drives the cost in perforated peptic ulcer
Insight into the history and trends of surgical simulation training in education: a bibliometric analysis
Surgical management of IBD—from an open to a laparoscopic approach
Laparoscopic appendicectomy in obese is associated with improvements in clinical outcome: systematic review

{kind=link}
{kind=link}