


Dear editor,
In 1975, Dr. Henry Heimlich introduced the Heimlich maneuver,[1] which has become the initial treatment for emergency foreign-body airway obstruction. It is recommended by American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care.[2] During thrusts, airway pressure increases, thereby expelling foreign bodies.
Generally, the Heimlich maneuver is safe and effective. Complications are rare, but they may be significant. In this study, we presented a case of blunt myocardial injury and gastrointestinal hemorrhage caused by this maneuver.
CASE
A 52-year-old deaf man with a history of hypertension experienced choking and became unconscious while eating noodle at supper. A nearby security guard performed the Heimlich maneuver. The noodle was dislodged. The patient regained consciousness and soon complained of upper abdominal discomfort.
He was brought to a local secondary hospital by ambulance 1 h later because of upper abdominal discomfort. Electrocardiography (ECG) results were normal during transportation. His vital signs on arrival were stable. Physical examination revealed periumbilical tenderness. Blood tests revealed an elevated lactate (Lac) level of 3.3 mmol/L (normal range 0.5-1.6 mmol/L). Further ECG, routine blood, coagulation, myocardial enzyme, and biochemical tests revealed normal results, except a low fibrinogen level of 1.16 g/L (normal range 2.0-4.0 g/L) and a high D-dimer level of 28,964 ng/mL (normal range ≤255 ng/mL). Abdominal computed tomography (CT) suggested dilation of the ascending colon and ileocecal area with more contents and accumulation of fluid inside the small intestine. The upper abdominal discomfort persisted, and the patient started to experience 10-50 mL hematochezia once every 30 min to 1 h. Ten hours after choking, the Lac level was 16 mmol/L. Ultrasound and CT suggested hydropericardium. Therefore, he was transferred to our hospital 12 h after choking.
On arrival at our hospital, a large tertiary teaching hospital in Beijing, his heart rate was 156 beats/min and blood pressure was 125/70 mmHg (1 mmHg=0.133 kPa). Physical examination revealed dilated jugular veins and cold extremities. ECG revealed abnormal findings with ST depression in leads II, III, aVF, and V5-6. Myocardial enzyme levels were elevated (myoglobin >500 ng/mL, troponin I 4.13 ng/mL). His hemoglobin level was stable. Ultrasound revealed a huge pericardial effusion with right ventricular regional wall motion abnormality (Figure 1). Acute cardiac tamponade and cardiogenic shock were diagnosed. Pericardiocentesis was performed, and 300 mL of blood was drained. His symptoms were greatly alleviated, and ECG showed normalization in leads II, III, and aVF. After this procedure, the patient could communicate with family members using sign language. Because hematochezia persisted during the procedure, injury to the colon was suspected, and conservative treatment was adopted.
Figure 1.
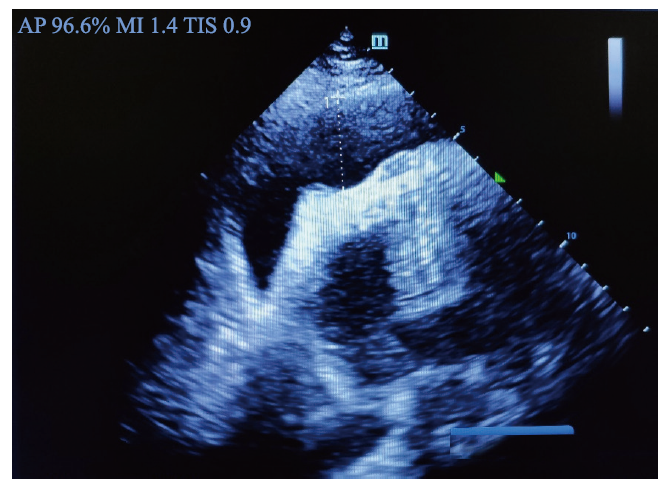
Figure 1.
Cardiac ultrasound. Cardiac ultrasound showed right ventricular regional wall motion abnormality.
Cardiac arrest occurred 18 h after choking (1.5 h after pericardiocentesis). Cardiotomy and internal cardiac massage were promptly performed at the bedside. The anterior wall of the right ventricle was extensively damaged (Figure 2); however, the other parts of the heart were normal. No signs of heart damage from pericardiocentesis were observed. The patient died 19 hours after choking.
Figure 2.
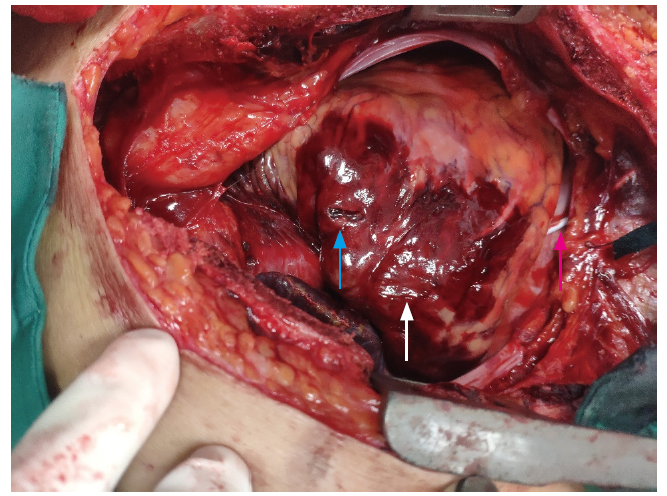
Figure 2.
Cardiotomy by bedside. Cardiotomy revealed extensively damage of the anterior wall of the right ventricle (the white arrow); the other parts of the heart were normal; the red arrow indicated the drainage tube; the blue arrow indicated a wound caused by cardiotomy.
DISCUSSION
Choking is an emergency that requires rapid recognition and treatment. The mortality rate due to choking is approximately 3.3%. The Heimlich maneuver is commonly used, with a success rate of 86.5%.[3] The main points of the Heimlich maneuver include the following: (1) stand behind the patient; (2) make a fist with one hand; (3) place the fist under the xiphoid process of the upper abdomen; and (4) make a quick, hard movement inward and upward.
Although the Heimlich maneuver is commonly considered a safe and effective way to remove foreign-body airway obstruction, the literature review showed that various complications (37 cases) were reported (supplementary Table 1). Complications occur mainly in the elderly population. Abdominal injuries (17 cases) were the most common, especially gastric rupture (11 cases), followed by aortic injuries (10 cases). Pancreatic injuries (two cases) occur mainly in young patients. No cases of blunt myocardial injury after the Heimlich maneuver have been reported.
During the maneuver, the mean peak airway pressure is approximately 26.4±19.8 cmH2O (1 cmH2O=0.098 kPa).[4] The pressure in the stomach can reach 57±17 cmH2O,[5] which is much higher than that in the airway. This partly explains why gastric rupture is the most common complication. Incorrect or improper implementation of the maneuver can successfully relieve airway obstruction, but can also cause direct trauma to the organs or tissues underneath, resulting in serious sequelae. In the case presented here, the heart and gastrointestinal tract were injured after the Heimlich maneuver, and the patient died 19 h after the choking episode.
Our literature review on complications after the Heimlich maneuver identified 37 cases. In these 37 cases, the Heimlich maneuver was performed by laypersons in 24 cases and by professionals in 10 cases. In three cases, the providers were unspecified. Healthcare professionals must be cautious when using the Heimlich maneuver. The indications for and techniques of the maneuver should be emphasized, especially the position of the fist on the abdomen and the direction of the force.
In addition, since the maneuver is often performed by laypersons, efforts should be directed toward instructing the public in the correct technique of the maneuver. Patients who undergo the Heimlich maneuver should be closely monitored for potential complications and further evaluated if symptoms develop.
CONCLUSIONS
The Heimlich maneuver is safe and effective, but complications occur. Impropriate application of the maneuver may successfully relieve airway obstruction, but it could result in serious sequelae. The importance of the indications for and techniques of the maneuver should always be emphasized. Organs around the upper abdominal area could be injured during the Heimlich maneuver. Patients with symptoms after the Heimlich maneuver should be thoroughly evaluated. In addition, education concerning the Heimlich maneuver should be strict and clear for both laypeople and professionals. Patients who develop discomfort after the Heimlich maneuver should be closely monitored and evaluated.
Funding: The study was supported by National Key R&D Program (2018YFF0301103).
Ethical approval: Not needed.
Conflicts of interests: The authors declare that there is no conflict of interest.
Contributors: CW and ZZW contributed equally to the manuscript. CW and ZZW designed the research and wrote the paper. All authors contributed to the design and interpretation of the study and to further drafts. TBW is the guarantor.
All the supplementary files in this paper are available at http://wjem.com.cn.
Reference
A life-saving maneuver to prevent food-choking
DOI:10.1001/jama.1975.03260170034021 URL [Cited within: 1]
Part 5: adult basic life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
Empyema associated with vegetable foreign body aspiration
DOI:10.5847/wjem.j.1920-8642.2021.02.015 URL [Cited within: 1]
Airway pressure with chest compressions versus Heimlich manoeuvre in recently dead adults with complete airway obstruction
PMID:10767497
[Cited within: 1]

In a previous case report a standard chest compression successfully removed a foreign body from the airway after the Heimlich manoeuvre had failed. Based on this case, standard chest compressions and Heimlich manoeuvres were performed by emergency physicians on 12 unselected cadavers with a simulated complete airway obstruction in a randomised crossover design. The mean peak airway pressure was significantly lower with abdominal thrusts compared to chest compressions, 26.4+/-19.8 cmH(2)O versus 40.8+/-16.4 cmH(2)O, respectively (P=0.005, 95% confidence interval for the mean difference 5.3-23.4 cmH(2)O). Standard chest compressions therefore have the potential of being more effective than the Heimlich manoeuvre for the management of complete airway obstruction by a foreign body in an unconscious patient. Removal of the Heimlich manoeuvre from the resuscitation algorithm for unconscious patients with suspected airway obstruction will also simplify training.
Choking on a foreign body: a physiological study of the effectiveness of abdominal thrust manoeuvres to increase thoracic pressure
DOI:10.1136/thoraxjnl-2016-209540 URL [Cited within: 1]

{kind=link}
{kind=link}
{kind=link}
{kind=link}