


Radiologic imaging is a diagnostic tool that greatly affects patient outcomes,[1] and with the recent development of imaging technology, advanced imaging tests such as computed tomography (CT) have gained widespread accessibility in hospitals. In particular, CT is essential in the evaluation of patients in low-level emergency departments (EDs) because of its ability to answer clinical questions accurately and quickly.[2] Therefore, the frequency of patients who are transferred to high-level EDs for treatment after performing CT in a low-level ED is increasing.[3] Thus, it has become important for the patient’s treatment plan to immediately reconfirm the CT image of a transferred patient in the referred ED.[4]
However, previous studies conducted on patients visiting EDs reported significant discrepancies of interpretations between EDs for the same CT image.[3-6] If such a discrepancy is found in the ED, the clinical process could change, and the performance of additional imaging may be required, resulting in unnecessary radiation exposure and an increased cost burden on patients.[7] Moreover, additional imaging studies may lead to prolonged ED length of stay (LOS), in turn causing ED crowding, which can adversely affect the patient’s clinical results and reduce the patient’s satisfaction level.[8,9] Therefore, if the risk factors for discrepancies in the interpretation of CT images of transferred patients are identified in advance, the emergency physicians of the referred hospital could prepare for the changes in the treatment plan caused by the discrepancy. However, previous studies have not been able to reach a clear consensus on the risk factors for discrepancies in the interpretation of CT of transferred patients.[6,7,10,11] Several such risk factors have been recently reported, but systematic results on their identification are lacking.[12,13,14,15] Furthermore, no studies have identified how inconsistencies in outside image interpretation affect patient outcomes.[16,17]
Our tertiary ED has an emergency transfer coordination center (ETCC) which coordinates inter-hospital transfers. It provides an appropriate setting for research on the issue of discrepancies in the interpretation of CT. In this setting, the present study aims to identify the risk factors for discrepancies in the interpretation of CT images in patients transferred to a high-level ED and investigate their effects on ED clinical processes.
METHODS
This is a cross-sectional study based on prospectively collected data from an ETCC data bank at an urban tertiary teaching hospital in the Republic of Korea. This study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.
Our government health authorities designate EDs as level 1, level 2, or level 3, depending on the availability of medical human resources, emergency equipment, and medical services. By law, level 1 and level 2 EDs must have 24-hour emergency medical doctors.[18] The ETCC at our hospital is in a level 1 ED. This ED is located in northwest Seoul (capital of the Republic of Korea) and is responsible for the management of severe patients in its catchment area. Of the approximately 90,000 annual visits to this ED, about 4,000 are patients transferred from other hospitals by emergency medical service (EMS). Approximately 25% of all patients who visit the ED are admitted to our hospital.[19]
In this study, all patients aged 19 years or older who were transferred through the ETCC with CT images obtained from other hospitals between June 2018 and December 2018, were included.
The following cases were excluded: (1) those with CT images (obtained from other hospitals) not transferred to our picture archiving and communication system (PACS); (2) those who were not transferred through the ETCC.
The ETCC is developed to coordinate all emergency transfers to our ED. The ETCC has 6 coordinators and 12 board-certified emergency physicians, and operates 24 hours a day. Using a computerized system, the coordinator continuously monitors the hospital ward capability status, the availability of operating rooms, and the equipment needed for emergency treatment. Based on these data, the ETCC approves patient transfers and manages the related database as a single cohort, recording diagnosis, medical conditions, examination records, and basic information for all patients requested to be transferred from the primary hospital. In addition, for patients who undergo CT, scan time, modality subtype, contrast medium use, and interpretation of CT images from the referring ED are collected prospectively. Our ED has an external image interpretation system in which all external images are immediately sent to the PACS on patient arrival and interpreted by certified radiologists. Therefore, it is possible to immediately detect discrepancies and analyze how they affect the ED clinical process.
For a patient to be transferred to our ED, the coordinator collects the patient’s information, including CT results according to standard protocols, and shares this information, as well as that regarding availability of equipment and hospital bed space, with the emergency medical staff to obtain approval for the transfer. If the input of other departments is needed, the coordinator includes their feedback in the decision-making process. Once approved, the patient is sent to the ED by ambulance or other available means of transportation. The ETCC protocol mandates the approval of transfer provided there is sufficient capacity in the ED; the transfer is denied only when there is overcrowding in the ED or ICU or lack of the required specialist. If primary stabilization is considered a top priority, emergency transfers from catchment areas are approved regardless of the ED capacity.[19]
The study data were extracted from the ETCC transfer registry, which contained prospectively collected data regarding patient age, sex, ED visit time and date, transfer reasons, stage at the referring facility, and CT scan status (CT subtype, CT contrast, reader specialty, and time elapsed from CT scan to ED arrival). In addition, information after arrival at the referred ED was automatically collected through a clinical research analysis portal developed by the medical information department in our hospital.[20] All data were collected by authorized researchers and fed into the hospital information system; they were processed anonymously, with no missing data.
The primary outcome is the presence of discrepancies between the external interpretation and our hospital’s interpretation. A major discrepancy was defined as any disagreement with clinical significance and potential change to the patient treatment plan; a minor discrepancy as any disagreement with no clinical significance; no discrepancy was defined as the absence of disagreement in interpretation according to previous literature.[16] The classification of discrepancies was conducted by two board-certified emergency physicians blinded to the study by reviewing the interpretation records and the patient’s clinical course from medical records. Differences in opinions between the two reviewers (14 cases of inconsistency) were determined through discussion until consensus was reached. In modeling, both minor and major discrepancies were classified as discrepancies. To confirm the effect of discrepancies on the ED clinical process, the present study investigated the time from ED presentation to the disposition of the enrolled patients.
Categorical variables are reported as number and percentage, and continuous variables as mean±standard deviation. Differences between groups were assessed by the Student’s t-test for normally distributed variables and by the Mann-Whitney U-test for the other variables. The Chi-squared test was used to analyze categorical variables. P-values less than 0.05 were considered statistically significant. Multivariable logistic regression analysis was performed to identify the risk factors for the primary outcome. Since this study was designed retrospectively and was an exploratory study analyzed using logistic regression, the post power calculation was not performed. The determination of clinically significant factors was based on previous studies.[3,4,5] Analysis of the collected data was performed using SAS (version 9.4, SAS Inc., USA) and R (version 3.6.3, http://www.R-project.org).
RESULTS
During the study period, 1,068 transfer requests out of a total of 2,837 were approved by the ETCC. There were 411 patients with outside CT images. Among them, 50 were excluded based on the exclusion criteria, resulting in the enrollment of 361 patients (Figure 1). A total of 107 (29.6%) cases were classified as discrepancies, among which 55 (15.24% of the total cases) were major discrepancies. Major discrepancies were present in 10 (11.36%) patients from high-level hospitals and 45 (16.48%) patients from low-level hospitals. Major discrepancies were found in 40 (23.95%) abdominal CT images and 3 (3.09%) brain CT images. The other baseline characteristics of the enrolled patients are shown in Table 1.
Figure 1.
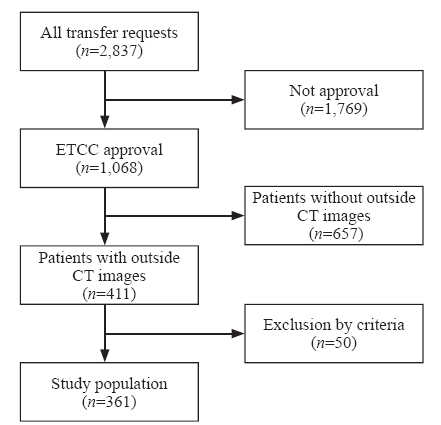
Figure 1.
Patient inclusion flowchart. ETCC: emergency transfer coordination center; CT: computed tomography.
Table 1 Patient characteristics according to discrepancy, n (%)
| Variables | No discrepancy (n=254) | Minor discrepancy (n=52) | Major discrepancy (n=55) |
|---|---|---|---|
| Age, years | 61.76±17.48 | 64.48±15.38 | 61.27±16.74 |
| Sex | |||
| Male (n=213) | 146 (68.54) | 38 (17.84) | 29 (13.62) |
| Female (n=148) | 108 (72.97) | 14 (9.46) | 26 (17.57) |
| Hospital level | |||
| High (n=88) | 61 (69.32) | 17 (19.32) | 10 (11.36) |
| Low (n=273) | 193 (70.70) | 35 (12.82) | 45 (16.48) |
| Trauma | |||
| Yes (n=83) | 67 (80.72) | 7 (8.43) | 9 (10.84) |
| No (n=120) | 187 (67.27) | 45 (16.19) | 46 (16.55) |
| CT | |||
| Multi (n=120) | 86 (71.67) | 22 (18.33) | 12 (10.00) |
| Single (n=241) | 168 (69.71) | 30 (12.45) | 43 (17.84) |
| Subtype | |||
| Abdominal (n=167) | 94 (56.29) | 33 (19.76) | 40 (23.95) |
| Brain (n=97) | 92 (94.85) | 2 (2.06) | 3 (3.09) |
| Chest (n=62) | 42 (67.74) | 14 (22.58) | 6 (9.68) |
| Others (n=35) | 26 (74.29) | 3 (8.57) | 6 (17.14) |
| Contrast medium | |||
| Not used (n=120) | 96 (80.00) | 17 (14.17) | 7 (5.83) |
| Used (n=241) | 158 (65.56) | 35 (14.52) | 48 (19.92) |
| Reader specialty | |||
| Radiologist (n=261) | 183 (70.12) | 39 (14.94) | 39 (14.94) |
| Others a (n=100) | 71 (71.00) | 13 (13.00) | 16 (16.00) |
| CT to door time b (hours) | 11.03±25.97 | 13.84±25.29 | 21.33±36.90 |
a: the reader is not a radiologist; b: the time from the completion of the CT scan to the final hospital arrival; Data are reported as mean±standard deviation or number (%). CT: computed tomography.
In univariable analyses, the presence of trauma, CT subtype, and use of contrast were identified as factors affecting discrepancies of interpretation, while in the multivariable model, the CT subtype was the only independent risk factor. In the univariable analyses, the odds ratio of non-trauma for discrepancies was 2.308 (95% confidence interval [CI] 1.118-3.714), and that of use of contrast was 2.101 (95% CI 1.249-3.535); these odds ratios changed to 1.643 (95% CI 0.727-3.715) and 0.957 (95% CI 0.501-1.829), respectively, in the multivariable logistic regression (Table 2). As part of the sensitivity analysis, we performed the multivariable logistic modeling of non-brain cases. In this analysis, no variable showed a significant effect on the discrepancy of CT image interpretation (supplementary file 1).
Table 2 Odds ratios for the discrepancy of CT interpretation
| Variables | Univariable analysis | Multivariable analysis | ||
|---|---|---|---|---|
| OR (95% CI) | P-value | OR (95% CI) | P-value | |
| Age, years | 1.004 (0.990-1.017) | 0.586 | 1.001 (0.987-1.017) | 0.848 |
| Sex | ||||
| Male | Ref | - | ||
| Female | 0.807 (0.507-1.284) | 0.365 | 0.736 (0.438-1.235) | 0.246 |
| Hospital level | ||||
| High | Ref | - | ||
| Low | 0.936 (0.555-1.579) | 0.806 | 0.767 (0.423-1.393) | 0.384 |
| Trauma | ||||
| Yes | Ref | - | ||
| No | 2.308 (1.118-3.714) | 0.020 | 1.643 (0.727-3.715) | 0.233 |
| CT | ||||
| Multi | Ref | - | ||
| Single | 1.099 (0.678-1.781) | 0.701 | 0.821 (0.429-1.569) | 0.550 |
| Subtype | ||||
| Brain | Ref | - | ||
| Abdominal | 14.285 (5.522-36.954) | <0.001 | 14.366 (5.216-39.567) | <0.001 |
| Chest | 8.759 (3.079-24.923) | <0.001 | 8.400 (2.851-24.755) | 0.001 |
| Others | 6.367 (1.963-20.652) | 0.002 | 6.250 (1.851-21.109) | 0.003 |
| Contrast medium | ||||
| Not used | Ref | - | ||
| Used | 2.101 (1.249-3.535) | 0.005 | 0.957 (0.501-1.829) | 0.894 |
| Reader specialty | ||||
| Radiologist | Ref | - | ||
| Others a | 1.043 (0.629-1.732) | 0.870 | 0.752 (0.425-1.331) | 0.328 |
| CT to door time (hours) b | 1.008 (0.999-1.016) | 0.051 | 1.007 (0.999-1.015) | 0.103 |
a: the reader is not a radiologist; b: the time from the completion of the CT scan to the final hospital arrival; CT: computed tomography; CI: confidence interval.
Figure 2 shows how the discrepancy of interpretation influenced the time to disposition in the ED. The present study confirmed that the discrepancy of interpretation was significantly associated with the prolonged time to disposition in ED (P=0.005).
Figure 2.
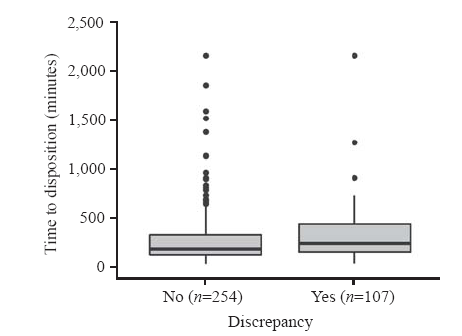
Figure 2.
Clinical effects of CT interpretation discrepancy.
DISCUSSION
Recently, due to the development of imaging technology, more patients are referred to high-level EDs after CT scans have been performed at primary medical institutions.[17] CT is a practical diagnostic tool, but is known to be affected by frequent interpretation discrepancies.[14] Accordingly, discrepancies in CT readings are of interest for many medical professionals. A previous study has shown that CT images are more consistent when the radiologist reads them, and that abdominal CT images can be read more accurately by radiologists.[15] Factors such as trauma image, age, and multiple CTs, which were assumed to be risk factors for discrepancies in CT image interpretation, were analyzed in previous studies. However, none of these studies were designed to target the discrepancy of interpretation of CT images performed on patients transferred between EDs, and were not performed using systematic methods.[7,11-14,17] In the present study, the interpretation of brain CT images was found to be relatively less inconsistent than that of other CT subtypes. The lower discrepancy rate of brain CT was in agreement with the results of a previous study.[13] It is believed that brain CT has lower discrepancy rates because the spectrum required to cover ED practice is narrow compared to other CT subtypes. Acute lesions, which can be detected using brain CT in EDs, do not have a broad spectrum of interpretation and do not involve various organs and anatomical structures like abdominal or chest CT scans. In our study, trauma and the absence of contrast medium were associated with low discrepancies. However, among the cases where brain CT was taken, the proportion of trauma and non-contrast cases was high. Therefore, contrast agents and trauma might have acted as confounders in the relationship between CT subtype and discrepancy.
The present study found that the time to disposition was prolonged in the discrepancy group. The disagreement in CT interpretation of transferred patients can cause the performance of additional CT in the clinical process, lengthening the patient’s ED LOS. Therefore, it may be helpful to evaluate the related risk factors during the transfer coordination process, so that CT image discrepancies can be predicted in advance. Based on the results of the present study, outside abdominal or chest CT images should be interpreted through a secondary reading system in the ED. Moreover, the results suggest the need of a system for immediate inter-hospital image transmission and interpretation by qualified radiologists before patient arrival. These efforts may also contribute to the rapid and accurate ED process of emergent transferred patients and alleviate ED crowding.
The present study has several strengths over previous studies of similar topics. It features a homogenous study population that was consecutively extracted thanks to a systematic emergency transfer system.[19] This allowed the standardized collection of known data to be associated with discrepancies of CT interpretation in patients transferred from various medical institutions, thus allowing the collection of variables that were difficult to identify in previous studies. In addition, our radiologic interpretation system allowed external images to be quickly moved to the internal PACS, allowing them to be interpreted more effectively,[2] the qualified radiologists being able to confirm discrepancies 24 hours/day in our ED. The results of the secondary interpretation were immediately reflected in the clinical process of the ED, which was an optimal place to achieve the study objectives.
This study has several limitations. First, although a prospectively collected registry was used, there was a possibility of bias due to the retrospective design of the study. In addition, it is difficult to generalize the study results because of its single-center nature. Finally, the clinical outcomes evaluated in our study did not include those related to patient safety, such as mortality or complications related to discrepancies. Therefore, additional studies to verify the association between inconsistencies in CT interpretation and patient outcome should be considered.
CONCLUSIONS
The CT subtype is the strongest risk factor for discrepancies of outside CT interpretation in patients urgently transferred to a high-level ED. Our study results can be used as practical evidence to prepare for secondary interpretation of CT images and clinical planning in EDs when there is a request for emergency transfer from other facilities.
Funding: None.
Ethical approval: This study adhered to the STROBE statement and was approved by the institutional review board (approval number 44-2020-0458).
Conflicts of interests: No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Contributors: HSL and JM contributed equally to this work. All authors approved the final version.
The supplementary file in this paper is available at http://wjem.com.cn/EN/10.5847/wjem.j.1920-8642.2022.001.
Reference
Prognostic implications of comprehensive whole vessel plaque quantification using coronary computed tomography angiography
DOI:10.1016/j.jacasi.2021.05.003 URL [Cited within: 1]
Outside imaging in emergency department transfer patients: CD import reduces rates of subsequent imaging utilization
DOI:10.1148/radiol.11101956
PMID:21507903
[Cited within: 2]

To test the hypothesis that among emergency department (ED) transfer patients, CD import of outside examinations into the picture archiving and communication system (PACS) decreases imaging utilization in the subsequent 24 hours.Institutional review board approval was obtained for this HIPAA-compliant study, with waiver of informed consent for retrospective medical records review. In 1487 consecutive ED patients, CD import to PACS was attempted between February 1 and August 31, 2009. Subsequent rates of imaging performed within 24 hours of any CD import attempt were extracted from the electronic medical record and compared between two patient groups: those with successful CD import and those for whom CD import had failed. Rates of all subsequent imaging and of computed tomographic (CT) imaging alone were compared by using the Wilcoxon rank sum test. ED CT utilization in the successful-import group was compared with that in a historical control group of 254 consecutive ED patients transferred with outside hospital CDs between August 2007 and January 2008, prior to implementation of import procedures.CD import to PACS was successful in 78% (1161 of 1487) of patients. Successful CD import produced a 17% reduction (P <.001) in mean rates of all subsequent diagnostic imaging, from 3.30 to 2.74 examinations per patient in the failed-import and successful-import groups, respectively, and a 16% reduction (P =.01) in subsequent CT utilization from mean of 1.41 to 1.19 scans per patient in those respective groups. Compared with the historical control group, posttransfer utilization of CT in the ED was reduced by 29% (P <.001) from 1.18 (historical control group) to 0.84 (successful-import group) scans per patient.Among ED transfer patients, CD import of outside imaging from the sending institution into the receiving institution's PACS significantly decreased the rates of subsequent imaging utilization.© RSNA, 2011.
Accuracy of outside radiologists’ reports of computed tomography exams of emergently transferred patients
DOI:10.1007/s10140-017-1573-8
PMID:29282579
[Cited within: 3]
Growing numbers of patient with advanced imaging being transferred to trauma centers has resulted in increased numbers of outside CT scans received at trauma centers. This study examines the degree of agreement between community radiologists' interpretations of the CT scans of transferred patients and trauma center radiologists' reinterpretation.All CT scans of emergency transfer patients received over a 1 month period were reviewed by an emergency radiologist. Patients were classified as trauma or non-trauma and exams as neuro or non-neuro. Interpretive discrepancies between the emergency radiologist and community radiologist were classified as minor, moderate, or major. Major discrepancies were confirmed by review of a second emergency radiologist. Discrepancy rates were calculated on a per-patient and per exam basis.Six hundred twenty-seven CT scans of 326 patients were reviewed. Major discrepancies were encountered in 52 (16.0%, 95% CI 12.2-20.5) patients and 53 exams (8.5%, 95% CI 6.5-10.5). These were discovered in 46 trauma patients (21.6%, 95% CI 16.4-27.9) compared to six non-trauma patients (5.3%, 95% CI 2.2-11.7) (P < 0.001). A significant difference in the major discrepancy rate was also found between non-neuro and neuro exams (12.4 vs 3.3%, respectively, P < 0.001), primarily due to discrepancies in trauma patients, rather than non-trauma patients.Potentially management-changing interpretive changes affected 16% of transferred patients and 8.5% of CT exams over a 1 month period. Trauma center reinterpretations of community hospital CT scans of transferred patients provide valuable additional information to the clinical services caring for critically ill patients.
Effectiveness of second-opinion radiology consultations to reassess the cervical spine CT scans: a study on trauma patients referred to a tertiary-care hospital
DOI:10.5152/dir.2015.15003
PMID:26200483
[Cited within: 2]
A second opinion is a valuable resource in confirming proper medical diagnosis and treatment. This study evaluates the effectiveness of second-opinion radiology consultations to reassess the cervical spine computed tomography (CT) scans of the trauma patients referred to our hospital.Cervical spine CT scans of 301 consecutive adult trauma patients, who were referred to our hospital from outside institutions, were analyzed. The emergency radiologists at our institution completed the over-read reports on the CT images obtained at the outside facilities. A single radiologist compared the outside- and over-read reports and determined the discrepancy of the radiologic reports.Based on the outside reports, 31% of the CT scans had cervical traumatic injury. In 92% of patients, the first-read and the over-read reports had consistent radiologic findings. About 90% of the positive, and 93% of the negative radiologic findings, were reported consistently in the over-read reports. Our analysis showed that the over-read reporting resulted in reassurance of negative findings in 63%; confirmation of positive findings in 29%; clearing a false diagnosis in 3%; and detection of a missed diagnosis in 5%. A rescan was done in 80% of patients with inconsistent and 20% of patients with consistent findings (P < 0.05). The most common missed radiologic findings in the first-reports were transverse and spinous process fractures and the most common misdiagnoses were dens fractures.For a service offering second-opinion consultations on cervical spine trauma, review of outside CT studies improves diagnosis and benefits patient care.
Outside CT imaging among emergency department transfer patients
DOI:10.1016/j.jacr.2009.04.010 URL [Cited within: 1]
Abdominal and pelvic computed tomography (CT) interpretation: discrepancy rates among experienced radiologists
DOI:10.1007/s00330-010-1763-1
PMID:20336300
[Cited within: 2]
To assess the discrepancy rate for the interpretation of abdominal and pelvic computed tomography (CT) examinations among experienced radiologists.Ninety abdominal and pelvic CT examinations reported by three experienced radiologists who specialize in abdominal imaging were randomly selected from the radiological database. The same radiologists, blinded to previous interpretation, were asked to re-interpret 60 examinations: 30 of their previous interpretations and 30 interpreted by others. All reports were assessed for the degree of discrepancy between initial and repeat interpretations according to a three-level scoring system: no discrepancy, minor, or major discrepancy. Inter- and intrareader discrepancy rates and causes were evaluated.CT examinations included in the investigation were performed on 90 patients (43 men, mean age 59 years, SD 14, range 19-88) for the following indications: follow-up/evaluation of malignancy (69/90, 77%), pancreatitis (5/90, 6%), urinary tract stone (4/90, 4%) or other (12/90, 13%). Interobserver and intraobserver major discrepancy rates were 26 and 32%, respectively. Major discrepancies were due to missed findings, different opinions regarding interval change of clinically significant findings, and the presence of recommendation.Major discrepancy of between 26 and 32% was observed in the interpretation of abdominal and pelvic CT examinations.
Second opinion interpretations by specialty radiologists at a pediatric hospital: rate of disagreement and clinical implications
DOI:10.2214/AJR.11.7662 URL [Cited within: 3]
Violence toward emergency physicians: A prospective-descriptive study
DOI:10.5847/wjem.j.1920-8642.2021.02.005
PMID:33728003
[Cited within: 1]
The highest rate of workplace violence occurs in the health sector, although most cases remain unreported. Emergency services face the majority of these incidents for many reasons, such as the patient profile, long waiting time, and overcrowding. We aimed to determine the characteristics and causes of violence toward emergency physicians.The acts of violence toward emergency physicians over a one-year period were prospectively recorded. After a violent incident took place, a third party separately interviewed the physician exposed to the violent behavior and the perpetrator who displayed this behavior. We examined the perpetrator's reasons for violence, their demographic characteristics, and the medical complaints of patients involved in such events to determine the characteristics and causes of violence.Of the violent acts investigated, 85.1% were verbal, and most were directed toward male doctors by the young male relatives of the patients. More than half of the violent acts occurred within the 15 minutes of presentation to emergency service (60.5%) and at off-hours (69.4%). Concerning the health insurance, 20.4% of the cases were covered by the free green card system, and a small number of the perpetrators of violence lived in rural areas (38.2%). The most common reason for violent behavior was the patients' or their relatives' dissatisfaction with the examination or treatment method (38.2%).Appropriate communication should be established with the patients, and they should be adequately informed about the treatments and interventions to be performed in order to prevent possible acts of violence.Copyright: © World Journal of Emergency Medicine.
Determinants of patient satisfaction and willingness to return with emergency care
PMID:10783404
[Cited within: 1]
To identify emergency department process of care measures that are significantly associated with satisfaction and willingness to return.Patient satisfaction and willingness to return at 5 urban, teaching hospital EDs were assessed. Baseline questionnaire, chart review, and 10-day follow-up telephone interviews were performed, and 38 process of care measures and 30 patient characteristic were collected for each respondent. Overall satisfaction was modeled with ordinal logistic regression. Willingness to return was modeled with logistic regression.During a 1-month study period, 2,899 (84% of eligible) on-site questionnaires were completed. Telephone interviews were completed by 2,333 patients (80% of patients who completed a questionnaire). Patient-reported problems that were highly correlated with satisfaction included help not received when needed (odds ratio [OR] 0.345; 95% confidence interval [CI] 0.261 to 0.456), poor explanation of causes of problem (OR 0.434; 95% CI 0.345 to 0.546), not told about potential wait time (OR 0.479; 95% CI 0.399 to 0.577), not told when to resume normal activities (OR 0.691; 95% CI 0.531 to 0.901), poor explanation of test results (OR 0.647; 95% CI 0.495 to 0.845), and not told when to return to the ED (OR 0.656; 95% CI 0. 494 to 0.871). Other process of care measures correlated with satisfaction include nonacute triage status (OR 0.701, 95% CI 0.578 to 0.851) and number of treatments in the ED (OR 1.164 per treatment; 95% CI 1.073 to 1.263). Patient characteristics that significantly predicted less satisfaction included younger age and black race. Determinants of willingness to return include poor explanation of causes of problem (OR 0.328; 95% CI 0.217 to 0.495), unable to leave a message for family (OR 0.391; 95% CI 0.226 to 0. 677), not told about potential wait time (OR 0.561; 95% CI 0.381 to 0.825), poor explanation of test results (OR 0.541; 95% CI 0.347 to 0.846), and help not received when needed (OR 0.537; 95% CI 0.340 to 0.846). Patients with a chief complaint of hand laceration were less willing to return compared with a reference population of patients with abdominal pain. Willingness to return is strongly predicted by overall satisfaction (OR 2.601; 95% CI 2.292 to 2.951).These data identify specific process of care measures that are determinants of patient satisfaction and willingness to return. Efforts to increase patient satisfaction and willingness to return should focus on improving ED performance on these identified process measures.
Pretransfer CT scans are frequently performed, but rarely helpful in rural trauma systems
DOI:S0002-9610(17)30473-7
PMID:28967379
[Cited within: 1]
Rural trauma patients often undergo workup prior to transfer to a trauma center. Repeat and redundant imaging at the trauma center is common.Two hundred consecutive adult trauma patients transferred to a regional trauma center were retrospectively evaluated.197 patients met criteria. 152 underwent CT scan prior to transfer and CT was the indication for transfer in 88 patients (44.7%). One intervention was performed as a result of CT imaging. 84 patients (55.3%) received repeat CT imaging. There were no statistically significant differences in rates of CT imaging at the outside facility based on injury severity, mechanism of injury, or age. The most common reason for repeat CT scans was incomplete initial imaging. The ability to obtain initial imaging was not a significant factor.Repeat CT imaging in transferred trauma patients is very common. The majority of reimaging is done for incomplete initial imaging. Rural trauma systems may benefit from improved protocols for more efficient care.Copyright © 2017 Elsevier Inc. All rights reserved.
The discrepancy rate between preliminary and official reports of emergency radiology studies: a performance indicator and quality improvement method
DOI:10.1177/0284185114532922 URL [Cited within: 2]
Rate and reasons for repeat CT scanning in transferred trauma patients
PMID:28541855
[Cited within: 1]
To describe the reasons and additional radiation for CT scans repeated after transfer to a trauma center. Retrospective study of patients transferred to a trauma center. Patients had repeat CT if a CT of the same region was repeated at the trauma center's emergency department. Indications for repeat CT scanning were abstracted. Radiation dosage was calculated in millisieverts. A total of 370 had CT scans and were transferred. Mean age was 39.1 ± 28.0 years. Seventy-four [20.0%, 95% confidence interval (CI) 16.0-24.4%] had 103 CTs repeated. Adults (64/254, 25.2%) were more likely than children (10/116, 8.6%) to undergo repeat CT (difference 16.6%, 95% CI 9.2-24.0%). Types of CTs repeated included: head 48 (47%), face 6 (6%), cervical spine/neck 21 (20%), thoracolumbar spine 4 (4%), chest 4 (4%), and abdominal/pelvic 20 (19%). Reasons for repeat CT were outside CT unavailable 31 (42%), insufficient image quality/additional details needed 15 (20%), disease progression 16 (22%), unknown 10 (14%), and consult request unknown reason 2 (3%). Median dose for the repeat CT scans was 4.19 mSv (interquartile range 1.98, 6.28) and was 4.79 mSv (interquartile range 2.47, 8.22) when the CTs were unavailable. Effective dose of the repeat scans was greater than 10 mSv in 13 (3.5%) patients. Patients transferred to a trauma center often undergo repeat CT. The most common reason for repeated imaging was failure to transport original CT scans with the patient or images that were unable to be viewed. Trauma centers should work with their catchment areas to establish systems that ensure transfer of all radiographic imaging.
Emergency imaging discrepancy rates at a level 1 trauma center: identifying the most common on-call resident “misses”
DOI:10.1007/s10140-013-1146-4 URL [Cited within: 2]
CT in adults: systematic review and meta-analysis of interpretation discrepancy rates
DOI:10.1148/radiol.13131114 URL [Cited within: 3]
The clinical impact of subspecialized radiologist reinterpretation of abdominal imaging studies, with analysis of the types and relative frequency of interpretation discrepancies
DOI:10.1007/s00261-014-0140-y URL [Cited within: 2]
The accuracy of interpretation of emergency abdominal CT in adult patients who present with non-traumatic abdominal pain: results of a UK national audit
DOI:S0009-9260(16)30430-5
PMID:27927488
[Cited within: 2]
To evaluate major/minor discrepancy rates for provisional (initial) and addendum (supplementary senior review) emergency computed tomography (CT) reports in patients presenting with non-traumatic abdominal pain.Ethical approval for this type of study is not required in the UK. All radiology departments with an approved lead for audit registered with the Royal College of Radiologists were invited to participate in this retrospective audit. The first 50 consecutive patients (25 surgical, 25 non-surgical) who underwent emergency abdominal CT for non-traumatic abdominal pain in 2013 were included. Statistical analyses were performed to identify organisational and report/patient-related variables that might be associated with major discrepancy.One hundred and nine (58%) of 188 departments supplied data to the study with a total of 4,931 patients (2,568 surgical, 2,363 non-surgical). The audit standard for provisional report major discrepancy was achieved for registrars (target <10%, achieved 4.6%), for on-site consultants (target <5%, achieved 3.1%) and consultant addendum (target <5%, achieved 2.9%). Off-site reporters failed to meet the standard target (<5%, achieved 8.7% overall and 12.7% in surgical patients). The standard for patients coming to harm was not met in the surgical group (target <1%, achieved 1.5%) and was narrowly missed overall (target <1%, achieved 1%).This study should be used to provide impetus to improve aspects of out-of-hours CT reporting. Clear benefits of CT interpretation/review by on-site and more senior (consultant) radiologists have been demonstrated.Copyright © 2016 The Royal College of Radiologists. Published by Elsevier Ltd. All rights reserved.
Interobserver agreement in the interpretation of outpatient head CT scans in an academic neuroradiology practice
DOI:10.3174/ajnr.A4058 URL [Cited within: 3]
Association between deprivation status at community level and outcomes from out-of-hospital cardiac arrest: a nationwide observational study
DOI:10.1016/j.resuscitation.2010.10.023
PMID:21146280
[Cited within: 1]
We sought to examine the association between area deprivation and outcomes of out-of-hospital cardiac arrest in Korea.Data were obtained from the emergency medical service (EMS) system. A nationwide OHCA cohort database from January 2006 to December 2007 was constructed via hospital chart review and ambulance run sheet data. We enrolled all EMS-assessed OHCA victims and excluded cases without available hospital outcome data or residential address. The Carstairs index was used to categorize districts according to level of deprivation into five quintiles, from (Q1, the least deprived) to (Q5, the most deprived). Main outcomes were survival to hospital discharge, survival to admission, and return of spontaneous circulation (ROSC).34,227 patients were included. Initial rhythm, witnessed status, attempted bystander cardiopulmonary resuscitation (CPR), CPR by EMS, CPR in the emergency department (ED), and elapsed time interval significantly varied according to area deprivation level (p < 0.001). OHCA outcomes were consistently worse in the most deprived areas. The adjusted OR (95% CI) for survival to hospital discharge was 0.58 (0.45-0.77) in the most deprived areas compared to the least deprived areas.Community deprivation was strongly associated with survival among out-of-hospital cardiac arrest patients in Korea.Copyright © 2010 Elsevier Ireland Ltd. All rights reserved.
Effects of an emergency transfer coordination center on secondary overtriage in an emergency department
DOI:10.1016/j.ajem.2018.05.060 URL [Cited within: 3]
Postcontrast acute kidney injury after computed tomography pulmonary angiography for acute pulmonary embolism
DOI:10.1016/j.jemermed.2019.09.006 URL [Cited within: 1]

{kind=link}
{kind=link}
{kind=link}
{kind=link}