World Journal of Emergency Medicine ›› 2021, Vol. 12 ›› Issue (4): 274-280.doi: 10.5847/wjem.j.1920-8642.2021.04.004
• Orginal Articles • Previous Articles Next Articles
Shan-xiang Xu, Chun-shuang Wu, Shao-yun Liu, Xiao Lu( )
)
Received:2021-01-15
Accepted:2021-06-26
Online:2021-09-01
Published:2021-08-17
Contact:
Xiao Lu
E-mail:jill44840@zju.edu.cn
Shan-xiang Xu, Chun-shuang Wu, Shao-yun Liu, Xiao Lu. High-flow nasal cannula oxygen therapy and noninvasive ventilation for preventing extubation failure during weaning from mechanical ventilation assessed by lung ultrasound score: A single-center randomized study[J]. World Journal of Emergency Medicine, 2021, 12(4): 274-280.
Add to citation manager EndNote|Ris|BibTeX
URL: http://wjem.com.cn/EN/10.5847/wjem.j.1920-8642.2021.04.004

Figure 1.
Flowchart of the study. ICU: intensive care unit; LUS: lung ultrasound score; NIV: noninvasive ventilation; HFNCO2: high-flow nasal cannula oxygen.
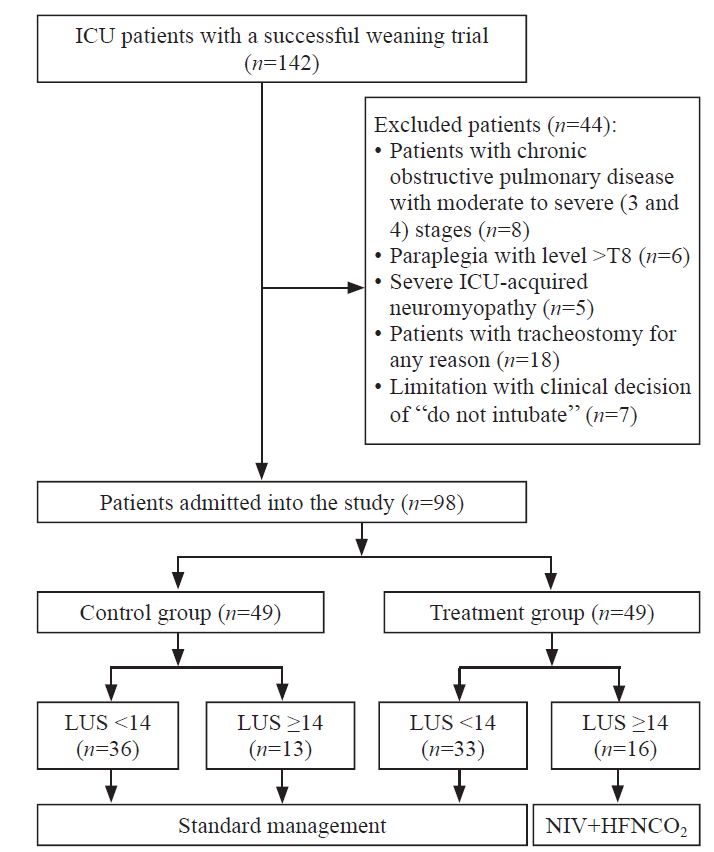
Table 1
Characteristics of the study participants at baseline
| Parameter | All patients (n=98) | Control group (n=49) | Treatment group (n=49) | P-value |
|---|---|---|---|---|
| Age (years) | 45±14 | 47±10 | 44±15 | 0.36 |
| Sex (male/female) | 52/47 | 28/20 | 24/27 | 0.43 |
| BMI (kg/m2) | 21.4±2.4 | 21.8±4.4 | 20.2±2.5 | 0.41 |
| SOFA score | 11.1±2.2 | 10.1±3.1 | 11.7±2.7 | 0.33 |
| LUS | 12.1±3.1 | 11.3±3.3 | 12.6±2.6 | 0.71 |
| Reason for ventilation/intubation, n (%) | ||||
| Severe trauma | 51 (52.0) | 23 (46.9) | 28 (57.1) | |
| Surgical emergency | 22 (22.4) | 12 (24.5) | 10 (20.4) | |
| Pneumonia | 12 (12.2) | 7 (14.3) | 5 (10.2) | |
| Extrapulmonary sepsis | 4 (4.1) | 1 (2.0) | 3 (6.1) | |
| Aspiration or drowning | 5 (5.1) | 2 (4.1) | 3 (6.1) | |
| Other | 4 (4.1) | 2 (4.1) | 2 (4.1) | |
| Re-intubation rate within 48 hours, n (%) | 14 (14.3) | 9 (18.4) | 5 (10.2) | <0.05 |
| Re-intubation rate within seven days, n(%) | 17 (17.3) | 11 (22.4) | 6 (12.2) | <0.05 |
| Time of ICU stay (days) | 8.5±3.5 | 9.4±3.1 | 7.2±2.4 | <0.05 |
| Duration of invasive mechanical ventilation before inclusion (days) | 6.4±1.7 | 6.5±1.4 | 6.2±2.1 | 0.73 |
| 28-day mortality, n (%) | 7 (7.1) | 3 (6.1) | 4 (8.2) | 0.87 |
Table 2
Evolution of respiratory parameters among patients with an LUS score ≥14 points
| Variables | Control group (n=13) | Treatment group (n=16) | P-value |
|---|---|---|---|
| H0 (end of weaning trial) | |||
| Respiratory rate, breaths/minute | 27±5 | 26±5 | 0.67 |
| Pulse rate, beats/minute | 105±13 | 110±11 | 0.43 |
| MAP, mmHg | 69±11 | 72±8 | 0.64 |
| pH | 7.33±0.21 | 7.37±0.5 | 0.44 |
| PaCO2, mmHg | 43.7±4.8 | 44.2±6.1 | 0.76 |
| PaO2/FiO2 | 213.6±27.5 | 225.5±32.8 | 0.25 |
| SPO2, % | 95.1±2.1 | 96.2±2.2 | 0.47 |
| H24 (24 hours after extubation) | |||
| Respiratory rate, breaths/minute | 23±2 | 20±2 | <0.05 |
| Pulse rate, beats/minute | 109±12 | 94±11 | <0.05 |
| MAP, mmHg | 77±13 | 82±12 | 0.33 |
| pH | 7.41±0.21 | 7.39±0.13 | 0.32 |
| PaCO2, mmHg | 41.3±3.7 | 38.1±3.1 | 0.45 |
| PaO2/FiO2 | 205.5±38.1 | 225.8±54.6 | <0.01 |
| SPO2, % | 94.8±2.6 | 97.9±1.1 | <0.05 |
| H48 (48 hours after extubation) | |||
| Respiratory rate, breaths/minute | 25±3 | 19±4 | <0.05 |
| Pulse rate, beats/minute | 110±18 | 87±12 | <0.05 |
| MAP, mmHg | 79±8 | 81±9 | 0.56 |
| pH | 7.44±0.14 | 7.41±0.16 | 0.24 |
| PaCO2, mmHg | 41.0±5.7 | 38.9±9.9 | 0.96 |
| PaO2/FiO2 | 207.3±43.9 | 262.6±59.1 | <0.01 |
| SPO2, % | 95.4±2.6 | 97.7±1.9 | <0.05 |
Table 3
Evolution of respiratory parameters among patients with an LUS score <14 points
| Variables | Control group (n=36) | Treatment group (n=33) | P-value |
|---|---|---|---|
| H0 (end of weaning trial) | |||
| Respiratory rate, breaths/minute | 23±5 | 25±4 | 0.33 |
| Pulse rate, beats/minute | 98±13 | 103±15 | 0.78 |
| MAP, mmHg | 73±10 | 78±11 | 0.25 |
| pH | 7.36±0.31 | 7.33±0.25 | 0.44 |
| PaCO2, mmHg | 42.1±3.5 | 39.2±6.1 | 0.36 |
| PaO2/FiO2 | 189.6±45.5 | 194.5±41.3 | 0.57 |
| SPO2, % | 96.2±3.1 | 97.1±2.2 | 0.38 |
| H24 (24 hours after extubation) | |||
| Respiratory rate, breaths/minute | 23±5 | 24±4 | 0.65 |
| Pulse rate, beats/minute | 111±16 | 109±15 | 0.33 |
| MAP, mmHg | 75±7 | 77±11 | 0.42 |
| pH | 7.31±0.55 | 7.34±0.45 | 0.56 |
| PaCO2, mmHg | 46.4±4.7 | 47.7±6.1 | 0.45 |
| PaO2/FiO2 | 200.1±78.6 | 192.8±44.6 | 0.67 |
| SPO2, % | 97.2±2.1 | 96.1±3.2 | 0.35 |
| H48 (48 hours after extubation) | |||
| Respiratory rate, breaths/minute | 22±4 | 21±4 | 0.57 |
| Pulse rate, beats/minute | 89±12 | 93±11 | 0.45 |
| MAP, mmHg | 78±7 | 80±7 | 0.78 |
| pH | 7.44±0.25 | 7.39±0.34 | 0.66 |
| PaCO2, mmHg | 41.1±3.3 | 45.9±3.4 | 0.13 |
| PaO2/FiO2 | 214.1±67.9 | 211.6±45.8 | 0.76 |
| SPO2, % | 98.1±1.4 | 98.0±1.2 | 0.88 |
| 1 |
Peñuelas O, Frutos-Vivar F, Fernández C, Anzueto A, Epstein SK, Apezteguía C, et al. Characteristics and outcomes of ventilated patients according to time to liberation from mechanical ventilation. Am J Respir Crit Care Med. 2011; 184(4):430-7.
doi: 10.1164/rccm.201011-1887OC |
| 2 |
Esteban A, Anzueto A, Frutos F, Alía I, Brochard L, Stewart TE, et al. Characteristics and outcomes in adult patients receiving mechanical ventilation: a 28-day international study. JAMA. 2002; 287(3):345-55.
doi: 10.1001/jama.287.3.345 |
| 3 |
Boles JM, Bion J, Connors A, Herridge M, Marsh B, Melot C, et al. Weaning from mechanical ventilation. Eur Respir J. 2007; 29(5):1033-56.
pmid: 17470624 |
| 4 |
Bouhemad B, Liu ZH, Arbelot C, Zhang M, Ferarri F, Le-Guen M, et al. Ultrasound assessment of antibiotic-induced pulmonary reaeration in ventilator-associated pneumonia. Crit Care Med. 2010; 38(1):84-92.
doi: 10.1097/CCM.0b013e3181b08cdb pmid: 19633538 |
| 5 |
Bouhemad B, Brisson H, Le-Guen M, Arbelot C, Lu Q, Rouby JJ. Bedside ultrasound assessment of positive end-expiratory pressure-induced lung recruitment. Am J Respir Crit Care Med. 2011; 183(3):341-7.
doi: 10.1164/rccm.201003-0369OC |
| 6 |
Wang YM, Zheng YJ, Chen Y, Huang YC, Chen WW, Ji R, et al. Effects of fluid balance on prognosis of acute respiratory distress syndrome patients secondary to sepsis. World J Emerg Med. 2020; 11(4):216-22.
doi: 10.5847/wjem.j.1920-8642.2020.04.003 |
| 7 |
Bouhemad B, Zhang M, Lu Q, Rouby JJ. Clinical review: bedside lung ultrasound in critical care practice. Crit Care. 2007; 11(1):205.
pmid: 17316468 |
| 8 |
Lichtenstein D, Goldstein I, Mourgeon E, Cluzel P, Grenier P, Rouby JJ. Comparative diagnostic performances of auscultation, chest radiography, and lung ultrasonography in acute respiratory distress syndrome. Anesthesiology. 2004; 100(1):9-15.
pmid: 14695718 |
| 9 |
Huang HW, Sun XM, Shi ZH, Chen GQ, Chen L, Friedrich JO, et al. Effect of high-flow nasal Cannula oxygen therapy versus conventional oxygen therapy and noninvasive ventilation on reintubation rate in adult patients after extubation: a systematic review and meta-analysis of randomized controlled trials. J Intensive Care Med. 2018; 33(11):609-23.
doi: 10.1177/0885066617705118 pmid: 28429603 |
| 10 |
Hernández G, Vaquero C, Colinas L, Cuena R, González P, Canabal A, et al. Effect of postextubation high-flow nasal Cannula vs noninvasive ventilation on reintubation and postextubation respiratory failure in high-risk patients: a randomized clinical trial. JAMA. 2016; 316(15):1565-74.
doi: 10.1001/jama.2016.14194 pmid: 27706464 |
| 11 |
Spoletini G, Garpestad E, Hill NS. High-flow nasal oxygen or noninvasive ventilation for postextubation hypoxemia: flow vs pressure? JAMA. 2016; 315(13):1340-2.
doi: 10.1001/jama.2016.2709 pmid: 26976699 |
| 12 |
Martins Tomazini B, Besen BAMP. High-flow oxygen vs noninvasive ventilation for postextubation respiratory failure. JAMA. 2017; 317(8):855.
doi: 10.1001/jama.2016.20986 pmid: 28245313 |
| 13 |
Jubran A, Lawm G, Kelly J, Duffner LA, Gungor G, Collins EG, et al. Depressive disorders during weaning from prolonged mechanical ventilation. Intensive Care Med. 2010; 36(5):828-35.
doi: 10.1007/s00134-010-1842-4 pmid: 20232042 |
| 14 |
Maggiore SM, Idone FA, Vaschetto R, Festa R, Cataldo A, Antonicelli F, et al. Nasal high-flow versus venturi mask oxygen therapy after extubation. Effects on oxygenation, comfort, and clinical outcome. Am J Respir Crit Care Med. 2014; 190(3):282-8.
doi: 10.1164/rccm.201402-0364OC |
| 15 |
Antonicelli F, Cataldo A, Festa R, Idone F, Moccaldo A, Antonelli M, et al. High-flow oxygen therapy through nasal cannulae versus low-flow oxygen therapy via Venturi mask after extubation in adult, critically ill patients. Crit Care. 2011; 15(suppl 1):165.
doi: 10.1186/cc10238 |
| 16 |
Bell N, Hutchinson CL, Green TC, Rogan E, Bein KJ, Dinh MM. Randomised control trial of humidified high flow nasal cannulae versus standard oxygen in the emergency department. Emerg Med Australas. 2015; 27(6):537-41.
doi: 10.1111/1742-6723.12490 |
| 17 |
Spoletini G, Garpestad E, Hill NS. High-flow nasal oxygen or noninvasive ventilation for postextubation hypoxemia: flow vs pressure? JAMA. 2016; 315(13):1340-2.
doi: 10.1001/jama.2016.2709 pmid: 26976699 |
| 18 |
Kulkarni AP, Agarwal V. Extubation failure in intensive care unit: predictors and management. Indian J Crit Care Med. 2008; 12(1):1-9.
doi: 10.4103/0972-5229.40942 |
| 19 |
Torres A, Gatell JM, Aznar E, El-Ebiary M, Puig de la Bellacasa J, González J, et al. Re-intubation increases the risk of nosocomial pneumonia in patients needing mechanical ventilation. Am J Respir Crit Care Med. 1995; 152(1):137-41.
doi: 10.1164/ajrccm.152.1.7599812 |
| 20 |
Vassilakopoulos T. Ventilator-induced diaphragm dysfunction: the clinical relevance of animal models. Intensive Care Med. 2008; 34(1):7-16.
doi: 10.1007/s00134-007-0866-x |
| 21 |
Petrof BJ, Jaber S, Matecki S. Ventilator-induced diaphragmatic dysfunction. Curr Opin Crit Care. 2010; 16(1):19-25.
doi: 10.1097/MCC.0b013e328334b166 pmid: 19935062 |
| 22 |
Coudroy R, Marjanovic N, Frat JP, Thille AW. Beneficial effects of noninvasive ventilation in acute hypoxemic respiratory failure: caution with findings from meta-analyses. Crit Care Med. 2017; 45(10):e1100-e1101.
doi: 10.1097/CCM.0000000000002567 |
| 23 |
Fernandez R, Subira C, Frutos-Vivar F, Rialp G, Laborda C, Masclans JR, et al. High-flow nasal Cannula to prevent postextubation respiratory failure in high-risk non-hypercapnic patients: a randomized multicenter trial. Ann Intensive Care. 2017; 7(1):47.
doi: 10.1186/s13613-017-0270-9 pmid: 28466461 |
| 24 |
Ou X, Hua Y, Liu J, Gong C, Zhao W. Effect of high-flow nasal Cannula oxygen therapy in adults with acute hypoxemic respiratory failure: a meta-analysis of randomized controlled trials. CMAJ. 2017; 189(7):E260-7.
doi: 10.1503/cmaj.160570 |
| 25 |
Kuang ZS, Yang YL, Wei W, Wang JL, Long XY, Li KY, et al. Clinical characteristics and prognosis of community-acquired pneumonia in autoimmune disease-induced immunocompromised host: a retrospective observational study. World J Emerg Med. 2020; 11(3):145-51.
doi: 10.5847/wjem.j.1920-8642.2020.03.003 |
| 26 |
Burns KE, Adhikari NK, Keenan SP, Meade M. Use of non-invasive ventilation to wean critically ill adults off invasive ventilation: meta-analysis and systematic review. BMJ. 2009; 338:b1574.
doi: 10.1136/bmj.b1574 |
| 27 |
Girault C, Bubenheim M, Abroug F, Diehl JL, Elatrous S, Beuret P, et al. Noninvasive ventilation and weaning in patients with chronic hypercapnic respiratory failure: a randomized multicenter trial. Am J Respir Crit Care Med. 2011; 184(6):672-9.
doi: 10.1164/rccm.201101-0035OC |
| 28 |
Chiumello D, Chevallard G, Gregoretti C. Non-invasive ventilation in postoperative patients: a systematic review. Intensive Care Med. 2011; 37(6):918-29.
doi: 10.1007/s00134-011-2210-8 pmid: 21424246 |
| 29 | Su CL, Chiang LL, Yang SH, Lin HI, Cheng KC, Huang YC, et al. Preventive use of noninvasive ventilation after extubation: a prospective, multicenter randomized controlled trial. Respir Care. 2012; 57(2):204-10. |
| 30 |
Ambrosino N, Vagheggini G. Noninvasive positive pressure ventilation in the acute care setting: where are we? Eur Respir J. 2008; 31(4):874-86.
doi: 10.1183/09031936.00143507 pmid: 18378782 |
| 31 |
Esteban A, Frutos-Vivar F, Ferguson ND, Arabi Y, Apezteguía C, González M, et al. Noninvasive positive-pressure ventilation for respiratory failure after extubation. N Engl J Med. 2004; 350(24):2452-60.
doi: 10.1056/NEJMoa032736 |
| 32 |
Keenan SP, Powers C, McCormack DG, Block G. Noninvasive positive-pressure ventilation for postextubation respiratory distress. JAMA. 2002; 287(24):3238.
doi: 10.1001/jama.287.24.3238 |
| [1] | Xue-xue Pu, Jiong Wang, Xue-bo Yan, Xue-qin Jiang. Sequential invasive-noninvasive mechanical ventilation weaning strategy for patients after tracheostomy [J]. World Journal of Emergency Medicine, 2015, 6(3): 196-200. |
| [2] | Rong-rong Song, Yan-ping Qiu, Yong-ju Chen, Yong Ji. Application of fiberoptic bronchscopy in patients with acute exacerbations of chronic obstructive pulmonary disease during sequential weaning of invasive-noninvasive mechanical ventilation [J]. World Journal of Emergency Medicine, 2012, 3(1): 29-34. |
| [3] | Huan Huang, Xin-hui Xu, Yi Chen, Li-xiong Lu, Chang-qing Zhu. Early tracheotomy for acute severe asthma [J]. World Journal of Emergency Medicine, 2011, 2(2): 154-156. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
