World Journal of Emergency Medicine ›› 2016, Vol. 7 ›› Issue (1): 40-43.doi: 10.5847/wjem.j.1920-8642.2016.01.007
• Original Articles • Previous Articles Next Articles
Deepak Geetaprasad Mishra1( ), Tamorish Kole1, Rahul Nagpal2, Jeffery Paul Smith3
), Tamorish Kole1, Rahul Nagpal2, Jeffery Paul Smith3
Received:2015-07-25
Accepted:2015-12-28
Online:2016-03-15
Published:2016-03-15
Contact:
Deepak Geetaprasad Mishra
E-mail:dr.deepak@hotmail.com
Deepak Geetaprasad Mishra, Tamorish Kole, Rahul Nagpal, Jeffery Paul Smith. A correlation analysis of Broselow™ Pediatric Emergency Tape-determined pediatric weight with actual pediatric weight in India[J]. World Journal of Emergency Medicine, 2016, 7(1): 40-43.
Add to citation manager EndNote|Ris|BibTeX
URL: http://wjem.com.cn//EN/10.5847/wjem.j.1920-8642.2016.01.007
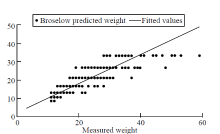
Figure 1.
Regression analysis of measured weight versus Broselow? Pediatric Emergency Tape-predicted weight for 603 Indian children.

Table 1
Patient characteristics
| Variables | Broselow-predicted weight groups (kg) | ||
|---|---|---|---|
| <10 kg (n=190) | 10-18 kg (n=224) | >18 kg (n=189) | |
| Age range (month) | 1-28 | 8-114 | 49-156 |
| Mean age* (month) | 6.54±6.69 | 32.61±15.89 | 83.01±25.20 |
| Females, n (%) | 89 (46.84) | 91 (40.63) | 77 (40.74) |
Table 2
Total agreement between Broselow? color-coding and actual weight in all patients, n (%)
| Variables | Broselow tape color-code zone | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Grey zone | Pink zone | Red zone | Purple zone | Yellow zone | White zone | Blue zone | Orange zone | Green zone | |
| Patients with correct prediction | 46 (76.67) | 24 (72.73) | 48 (75.00) | 54 (60.67) | 63 (65.63) | 58 (57.43) | 45 (64.29) | 28 (51.85) | 15 (44.12) |

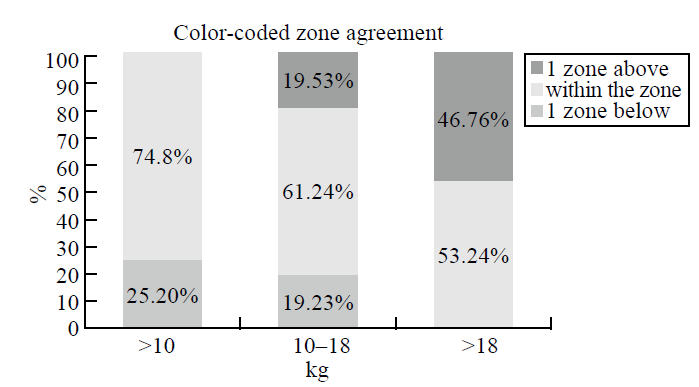
Figure 2.
Color-coded zone agreement for each weight group.
| 1 |
Anglemyer BL, Hernandez C, Brice JH, Zou B. The accuracy of visual estimation of body weight in the ED. Am J Emerg Med 2004; 22:526-529.
doi: 10.1016/j.ajem.2004.09.002 |
| 2 |
Harris M, Patterson J, Morse J. Doctors, nurses, and parents are equally poor at estimating pediatric weights. Pediatr Emerg Care 1999; 15:17-18.
pmid: 10069305 |
| 3 | Broselow J, Luten R, inventors; Vital Signs, Inc, assignee. Broselow pediatric emergency tape. US patents 4 713 888, December 22, 1987; 4 823 469, April 25, 1989; and 5 010 656, April 30, 1991. |
| 4 | Potts MJ, Phelan KW. Deficiencies in calculation and applied mathematics skills in pediatrics among primary care interns. Arch Pediatr Adolesc Med 1996; 150:748-752. |
| 5 | Rowe C, Koren T, Koren G. Errors by paediatric residents in calculating drug doses. Arch Dis Child 1998; 79:56-58. |
| 6 | Lesar TS. Errors in the use of medication dosage equations. Arch Pediatr Adolesc Med 1998; 152:340-344. |
| 7 | Koren G, Barzilay Z, Greenwald M. Tenfold errors in administration of drug doses: a neglected iatrogenic disease in pediatrics. Pediatrics 1986; 77:848-849. |
| 8 |
Thomas EJ, Studdert DM, Burstin HR, Orav EJ, Zeena T, Williams EJ, et al. Incidence and types of adverse events and negligent care in Utah and Colorado. Med Care 2000; 38:261-271.
pmid: 10718351 |
| 9 |
Leape LL, Brennan TA, Laird N, Lawthers AG, Localio AR, Barnes BA, et al. The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II. N Engl J Med 1991; 324:377-384.
pmid: 1824793 |
| 10 | Bates DW, Cullen DJ, Laird N, Petersen LA, Small SD, Servi D, et al. Incidence of adverse drug events and potential adverse drug events. Implications for prevention. ADE Prevention Study Group. JAMA 1995; 274:29-34. |
| 11 | Leape LL, Bates DW, Cullen DJ, Cooper J, Demonaco HJ, Gallivan T, et al. Systems analysis of adverse drug events. ADE Prevention Study Group. JAMA 1995; 274:35-43. |
| 12 |
Kaushal R, Bates DW, Landrigan C, McKenna KJ, Clapp MD, Federico F, et al. Medication errors and adverse drug events in pediatric inpatients. JAMA 2001; 285:2114-2120.
pmid: 11311101 |
| 13 | Lesar TS, Lomaestro BM, Pohl H. Medication-prescribing errors in a teaching hospital. A 9-year experience. Arch Intern Med 1997; 157:1569-1576. |
| 14 |
Hofer CK, Ganter M, Tucci M, Klaghofer R, Zollinger A. How reliable is length-based determination of body weight and tracheal tube size in the paediatric age group? The Broselow tape reconsidered. Br J Anaesth 2002; 88:283-285.
pmid: 11878662 |
| 15 | Black K, Barnett P, Wolfe R, Young S. Are methods used to estimate weight in children accurate? Emerg Med (Fremantle) 2002; 14:160-165. |
| 16 |
Jang HY, Shin SD, Kwak YH. Can the Broselow tape be used to estimate weight and endotracheal tube size in Korean children? Acad Emerg Med 2007; 14:489-491.
pmid: 17384410 |
| 17 |
Ramarajan N, Krishnamoorthi R, Strehlow M, Quinn J, Mahadevan SV. Internationalizing the Broselow tape: how reliable is weight estimation in Indian children. Acad Emerg Med 2008; 15:431-436.
pmid: 18439198 |
| 18 |
Shah AN, Frush K, Luo X, Wears RL. Effect of an intervention standardization system on pediatric dosing and equipment size determination: a crossover trial involving simulated resuscitation events. Arch Pediatr Adolesc Med 2003; 157:229-236.
pmid: 12622671 |
| 19 |
Lubitz DS, Seidel JS, Chameides L, Luten RC, Zaritsky AL, Campbell FW. A rapid method for estimating weight and resuscitation drug dosages from length in the pediatric age group. Ann Emerg Med 1988; 17:576-581.
pmid: 3377285 |
| 20 | Gragnolati M, Shekar M, Das Gupta M, Bredenkamp C, Lee Y-K. India's undernourished children. A call for reform and action. Health, Nutrition and Population (HNP) Discussion Paper. The World Bank. 2005 Aug. |
| 21 |
Bhandari N, Bahl R, Taneja S, de Onis M, Bhan MK. Growth performance of affluent Indian children is similar to that in developed countries. Bull World Health Organ 2002; 80:189-195.
pmid: 11984604 |
| 22 |
Varghese A, Vasudevan VK, Lewin S, Indumathi CK, Dinakar C, Rao SD. Do the length-based (Broselow) Tape, APLS, Argall and Nelson's formulae accurately estimate weight of Indian children? Indian Pediatr 2006; 43:889-894.
pmid: 17079832 |
| [1] | Alexei Birkun, Fatima Trunkwala, Adhish Gautam, Miriam Okoroanyanwu, Adesokan Oyewumi. Availability of basic life support courses for the general populations in India, Nigeria and the United Kingdom: An internet-based analysis [J]. World Journal of Emergency Medicine, 2020, 11(3): 133-139. |
| [2] | Muhammad Akhter Hamid, Ruqiya Afroz, Uqba Nawaz Ahmed, Aneela Bawani, Dilnasheen Khan, Rabia Shahab, Asim Salim. The importance of visualization of appendix on abdominal ultrasound for the diagnosis of appendicitis in children: A quality assessment review [J]. World Journal of Emergency Medicine, 2020, 11(3): 140-144. |
| [3] | Amar Pujari, Deepa R Swamy, Rashmi Singh, Ritika Mukhija, Rohan Chawla, Pradeep Sharma. Ultrasonographic assessment of paediatric ocular emergencies: A tertiary eye hospital based observation [J]. World Journal of Emergency Medicine, 2018, 9(4): 272-275. |
| [4] | Karun Shrestha, Prakriti Subedi, Oshna Pandey, Likhita Shakya, Kailash Chhetri, Darlene R. House. Estimating the weight of children in Nepal by Broselow, PAWPER XL and Mercy method [J]. World Journal of Emergency Medicine, 2018, 9(4): 276-281. |
| [5] | Hojjat Sheikhbardsiri, Mohammad H. Yarmohammadian, Fatemeh Rezaei, Mohammad Reza Maracy. Rehabilitation of vulnerable groups in emergencies and disasters: A systematic review [J]. World Journal of Emergency Medicine, 2017, 8(4): 253-263. |
| [6] | Muhammad Akhter Hamid, Sohaib Siddiqui, Jabeen Fayyaz, Ayesha Chandna, Aliya Ariz, Joe Butchey, Elancheliyan Ambalavanar, Niraj Mistry, Aftab Muhammad Azad, Junaid A. Bhatti, Dennis Scolnik. Paediatric-appropriate facilities in emergency departments of community hospitals in Ontario: A cross-sectional study [J]. World Journal of Emergency Medicine, 2017, 8(4): 264-268. |
| [7] | Emad Siddiqui, Badar Afzal, Ghazala Kazi, Asher Feroz, Rubaba Naeem, Tarab Mansoor, Ahreen Allana, Saif Siddiqui, Zain Siddiqui. Factors behind not using child restrain(t) among hospital employees and general population: A case control study [J]. World Journal of Emergency Medicine, 2017, 8(4): 269-275. |
| [8] | Linda Chokotho, Wakisa Mulwafu, Isaac Singini, Yasin Njalale, Kathryn H. Jacobsen. Improving hospital-based trauma care for road traffic injuries in Malawi [J]. World Journal of Emergency Medicine, 2017, 8(2): 85-90. |
| [9] | Thavinee Trainarongsakul, Pitsucha Sanguanwit, Supawan Rojcharoenchai, Kittisak Sawanyawisuth, Yuwares Sittichanbuncha. The RAMA Ped Card: Does it work for actual weight estimation in child patients at the emergency department [J]. World Journal of Emergency Medicine, 2017, 8(2): 126-130. |
| [10] | Vinej Somaraj, Rekha P Shenoy, Ganesh Shenoy Panchmal, Praveen S Jodalli, Laxminarayan Sonde, Ravichandra Karkal. Knowledge, attitude and anxiety pertaining to basic life support and medical emergencies among dental interns in Mangalore City, India [J]. World Journal of Emergency Medicine, 2017, 8(2): 131-135. |
| [11] | Chun Tat Lui. Prescription practice of antihistamines for acute upper respiratory tract infections in pediatric patients in a local emergency department in Hong Kong [J]. World Journal of Emergency Medicine, 2017, 8(1): 47-54. |
| [12] | Tigist Bacha, Birkneh Tilahun. A cross-sectional study of children with acute poisoning: A three-year retrospective analysis [J]. World Journal of Emergency Medicine, 2015, 6(4): 265-269. |
| [13] | Emaduddin Siddiqui, Kiran Ejaz, Shahan Waheed, Ghazala Irfan Kazi, Munawar Khursheed. Attitudes towards child restrains and seat belts usage in the learned population of Karachi, Pakistan [J]. World Journal of Emergency Medicine, 2014, 5(3): 223-228. |
| [14] | Anil Kumar Joshi, Chitra Joshi, Mridu Singh, Vikram Singh. Road traffic accidents in hilly regions of northern India: What has to be done? [J]. World Journal of Emergency Medicine, 2014, 5(2): 112-115. |
| [15] | Anish F James, Maya Jose. An academic emergency department:residents' perspective [J]. World Journal of Emergency Medicine, 2012, 3(1): 16-22. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
