World Journal of Emergency Medicine ›› 2017, Vol. 8 ›› Issue (4): 253-263.doi: 10.5847/wjem.j.1920-8642.2017.04.002
• Review Articles • Previous Articles Next Articles
Hojjat Sheikhbardsiri1, Mohammad H. Yarmohammadian2, Fatemeh Rezaei2, Mohammad Reza Maracy3( )
)
Received:2016-12-12
Accepted:2017-07-09
Online:2017-12-15
Published:2017-12-15
Contact:
Mohammad Reza Maracy
E-mail:mrmaracy@yahoo.co.uk
Hojjat Sheikhbardsiri, Mohammad H. Yarmohammadian, Fatemeh Rezaei, Mohammad Reza Maracy. Rehabilitation of vulnerable groups in emergencies and disasters: A systematic review[J]. World Journal of Emergency Medicine, 2017, 8(4): 253-263.
Add to citation manager EndNote|Ris|BibTeX
URL: http://wjem.com.cn//EN/10.5847/wjem.j.1920-8642.2017.04.002
Figure 1.
Flow diagram showing selection of articles reviewed, in accordance with the PRISMA Guidelines 10.
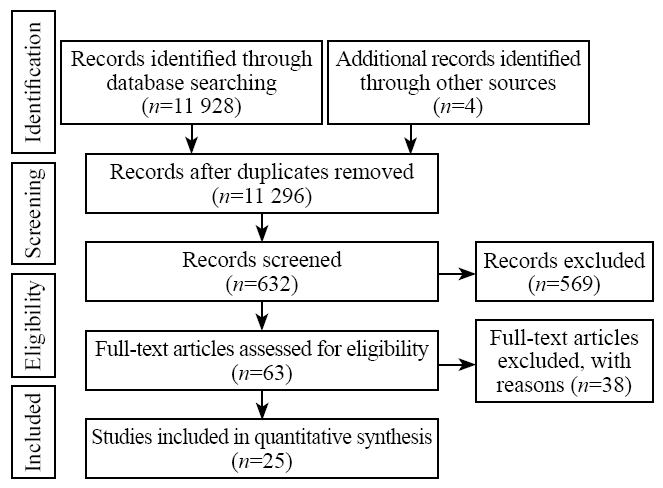
Table 1
The quality of the final extracted articles using Critical Appraisal Skills Program (CASP)[11,12]
| Randomized controlled trial | Clear focused issue | Adequate randomization procedure | Participants properly accounted | Blinding of participants/ assessors | Groups similar at start | Groups treated equally | Large treatment effect | Precise treatment effect | Clinically important outcomes considered | Benefits worth harms and costs | CASP Grade |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Berger et al[ | + | - | + | - | - | - | + | + | + | - | 5/10 |
| Zhang et al[ | + | - | + | - | - | + | - | - | + | + | 5/10 |
| Zang et al[ | + | + | + | - | + | + | + | + | + | - | 8/10 |
| Cross-sectional studies | Clear focused issue | Appropriate method | Appropriate cohort recruitment | Exposure accurately measured | Outcome accurately measured | Important confounding factors accounted | Adequate follow-up | Strong exposure and outcome relation | Precise results | Believe the results | CASP Grade |
| Edgar et al[ | + | - | - | + | + | - | + | + | + | - | 6/10 |
| Jothi et al[ | + | - | - | + | + | - | - | + | - | + | 5/10 |
| Becker[ | + | - | + | + | + | + | - | + | - | + | 5/10 |
| Chiou-Tan et al[ | + | + | - | - | + | - | - | + | - | + | 7/10 |
| Rauch et al[ | + | - | - | + | + | - | + | + | - | + | 6/10 |
| Becker[ | + | + | - | - | + | - | - | - | - | - | 3/10 |
| Math et al[ | + | + | - | - | + | - | + | - | - | + | 5/10 |
| Mallick et al[ | + | - | - | + | + | - | + | + | - | + | 6/10 |
| Raissi[ | + | - | - | + | + | - | - | - | - | - | 4/10 |
| Régnier et al[ | + | - | - | + | + | - | + | + | + | - | 6/10 |
| Rathore et al[ | + | - | - | + | + | - | - | + | + | + | 6/10 |
| Bazeghi et al[ | + | - | - | - | + | - | - | + | - | + | 4/10 |
| Ni et al[ | + | + | + | - | - | - | - | + | + | - | 5/10 |
| Xiao et al[ | + | - | + | - | - | - | + | + | - | - | 4/10 |
| Li et al[ | + | + | - | - | - | - | - | + | + | - | 4/10 |
| Tan et al[ | + | - | - | - | - | - | - | - | - | + | 2/10 |
| Qualitative studies | Study aim | Methodology | Study design | Sampling | Data collection | Reflexivity | Ethical issues | Data analysis | Findings | Value of the research | CAS Grade |
| Khankeh et al[ | + | + | + | + | + | - | - | + | + | + | 8/10 |
| Adams et al[ | + | + | - | - | - | - | - | + | - | - | 3/10 |
| Bazeghi et al[ | + | - | - | - | + | - | - | + | - | + | 4/10 |
| Mansoor et al[ | + | + | - | - | + | - | + | + | + | + | 7/10 |
| Larson et al[ | + | + | - | + | + | - | - | + | - | + | 6/10 |
| Huang et al[ | + | + | - | - | - | - | - | - | - | + | 3/10 |
Table 2
Summary of papers related to rehabilitation of vulnerable groups in emergencies and disasters
| Authors | Study type | Vulnerable group | Sample size | Disaster type | Location | Type rehabilitation | Setting | Post disaster (phase) | Duration | Main concept | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Natural | Man-made | |||||||||||||||||||||
| Qualitative studies analyzes | ||||||||||||||||||||||
| Khankeh et al[ | Qualitative | Women | 10 | Earthquake | Iran | Physical, psychological, social | Community | No detail | No detail | This study extracted the three following concepts: (1) needs for health recovery; (2) intent to delegate responsibility; and (3) desire for a wide scope of social support. One of the most important weaknesses of rehabilitations from participants' viewpoint was that after the response stage where people were rescued and discharged, there were no specialized centers to continue long-term rehabilitation activities. Also after the occurrence of a disaster, authorities' sensitiveness decreases and few disaster news was reported on the local media. Participants said that after disaster and destruction of their houses, they were kept in long-term shelters that could impose a variety of mental and psychological traumas. An important finding of this paper is that performing rehabilitation activities require cooperation from public and private sectors, and governmental organizations cannot conduct appropriate rehabilitation for injured individuals. Furthermore, local authorities' role in restoring the injured to pre-disaster conditions in total rehabilitation phase is of high importance. | ||||||||||||
| Adams et al[ | Qualitative | The elder | 165 | Hurricanes | United States | Social | No detail | No detail | No detail | Social rehabilitation activates include: older participants in treatment process and help to obtain authority and reinforcement, individual and family supports, communicate between resources and needs of the elderly and also help to access these resources, identify skills, competencies and specialization of elderly. Result of this article showed the elderly with high blood pressure, cardiac conditions, diabetes, kidney disease and cancer were unable to receive regular care. After Katrina hurricane many elderly people with chronic conditions did not get treatment for long periods of time; others were unable to receive regular checkups or obtain medications. Many elderly people died from lack of medication for chronic conditions, especially diabetes, hypertension, and asthma. | ||||||||||||
| Larson et al[ | Qualitative | Women | 57 | Tsunami | India | Social, economical | Affected setting | Long term | No detail | Rehabilitation activates include formation of self-help groups, consisting of 8 to 10 individuals. The major role was to decrease poverty disaster-affected women. Results showed that value and dignity of women and men were not the same before and after tsunami. Men worked and women just took care of children, but after formation of self-help groups following the tsunami, drastic changes occurred in women's roles; they could also work outside of the home. Increasing the number of self-help groups was a major rehabilitation activity which could get a huge amount of international humanitarian helps. Self-help groups offered low interest loans to the affected women. The good thing about this loan was that every family was paid with a monthly amount regarding their financial status. For social rehabilitation, women participate in development actives that designed based on social partnership, and identify skills and competencies in order to perform appropriate and correct social rehabilitation programs in families and society. | ||||||||||||
| Mansoor et al[ | Qualitative | Children | 18 | Flood, earthquake | Pakistan | Psychological | Orphanages | Long term | No detail | Disasters may have negative impacts on children who witnessed the tragedy and lost their family members. These negative impacts include sleep disorders, social isolation, and posttraumatic stress disorder. One of the most important results of this study was that there should not be any gap between response phase and rehabilitation phase for children. Since there is a gap, the rehabilitation procedures are difficult. Rehabilitation activities used for children include asking them to speak about their feelings and sadness. Children are generally interested to speak with others of their own age; therefore this opportunity should be provided for them to meet school friends and teachers that can decrease their anxiety and stress. | ||||||||||||
| Bazeghi et al[ | Qualitative | Children | 25 | Earthquake | Iran | Economical, social | Governmental and non-governmental in Iran | Long term | After disaster | The Iranian Red Crescent Organization, Emdad Imam Khomeini Committee (a national organization unique to Iran that is protected by the government and supported by public contributions) and Behzisti organization (the government welfare organization in Iran) are the main organizations involved in the management of separated and unaccompanied children, following disasters in Iran. NGOs are rarely responsible for caring for unaccompanied children; however they provide valuable support including financial assistance, arrangement of educational and extra-curricular activities, and psychosocial support like participating in art activities such as painting, embroidery, doll making for girls and various sports activities for boys such as football. | ||||||||||||
| Huang et al[ | Qualitative | The Older and women | 24 | Earthquake | China | Social | Community centers | Long term | Once a week (60-90 minutes); 9 total sessions | Social rehabilitation programs include: various group activities, promotion of harmony among members and fostered group leaders, and communication with other groups outside the community. Most participants indicated no distance in thinking about the earthquake. Women declared that joining the social group life was meaningful. After joining the group, participants' social networks were broadened and strengthened, and they recognized the importance of mutual understanding and developed a sense of cooperation. | ||||||||||||
| Cross-sectional studies analyzes | ||||||||||||||||||||||
| Jothi et al[ | Cross-sectional | Women | 200 | Tsunami | India | Social and educational | Affected community | 3-28 days | No detail | Nature of disasters can cause great changes in economic and psychological aspects of women's lives. This paper showed women preferred TV to other medias to know about disaster news. So, TV can play a major role in teaching social rehabilitating activities to injured individuals particularly women. The study found that one of the good points about TV was the first-hand information about disaster and its following rehabilitation activities. Another role of media was to identify and introduce centers and social supporting institutions, and also to advise and guide women's to social services related with health at the community level after disasters. | ||||||||||||
| Becker[ | Cross-sectional | Children and the elder | No detail | Tsunami | India | Psychological and social (educational) | Temporary housing camps | Long term | First 3 months after the disaster | Social and psychological rehabilitations activities for adults and children include: helping them talk about their feelings to others to correct their understanding from disaster, as well as accepting the changes to their bodies and mentalities caused by that incident; decreasing physical, psychological and social symptoms; strengthening relaxation; discharging excitements with using proper proverbs, and strengthening social cohesion through social activities and support group. Authorities held some group meetings with children at school to comfort their experiences, and created supporting groups to help them speak their anxiety about the loss of schools, teachers, and their academic records. | ||||||||||||
| Raissi[ | Case study | The disabled | 54 | Earthquake | Iran | Physical, educated (social) | Clinic, setting effected | 4-12 weeks | 3 months | This study reported important obstacles for physical rehabilitation procedures. These factors include: lack of accurate information, spreading the residents of Bam to other parts of the country, lack of skilled staff, loss of previous information due to earthquake, transferring the injured people for several times and destruction of addresses and maps. Another important finding is that a designed intervention of physical rehabilitation should be consider as the role of their participation. One of the important indicators which is proper to physical rehabilitation programs is that religious, social, cultural and economic factors should be considered for affected people. Not knowing cultural viewpoints of patients and lack of ability to communicate with them is the main weaknesses of rehabilitation service providers. So, training local staff and using them for providing physical rehabilitations activates can lead to providing better, faster services with lower cost and more longer term. | ||||||||||||
| Li et al[ | Prospective cohort study | Women | 51 | Earthquake | China | Physical | Hospital | 0-72 | 3 months | Most victims rescued from the debris within 30 minutes after the earthquake (70.6%), and all surviving victims rescued within 9 hours. 86.3% patients received surgical spinal stabilization; only 7 patients underwent surgery within 5 days after the earthquake. 94.1% patients began rehabilitation therapy within 4 months. 90% patients resumed to walk using outhouses; 90.2% used a wheelchair. Patient unadjusted/raw MBI scores improved significantly (mean difference, 29±16.9 points) during the rehabilitation program. At the end of therapy, 35% patients achieved moderate ADL independence, and 90.2% regained some self-care ability. Rehabilitation program was the strongest predictor of significantly increased MBI scores (increase of 34 points; 95%CI 28-41). Complications included bowel and bladder dysfunction (60.8% and 58.8%, respectively); 63% (pressure ulcers) to 85% (deep vein thrombosis). Earlier rescue and rehabilitation were significant positive predictors of rehabilitation effectiveness. Individualized rehabilitation program was provided by multidisciplinary rehabilitation team, comprised of physiatrists, therapists (physical, occupational, traditional modalities), rehabilitation nurses, volunteers, and other consulting medical specialists. Rehabilitation modalities included exercises, muscle strengthening, transfers, training ADL, and mobility training; ultrasound, functional electrical stimulation, electrotherapy, infrared, and lymphatic flow modalities; traditional Chinese therapies (acupuncture, massage); education in management of bladder and bowel continence, skin care, and self-exercise; and assistive devices (prostheses, orthoses) prescribed and provided if indicated. | ||||||||||||
| Xiao et al[ | Cross-sectional | Women | 174 | Earthquake | China | Physical | Hospital, rehabilitation facilities | 4-12 weeks | Two 40-minute sessions per day for >1 month | Rehabilitation interventions delivered by physiotherapists, which included muscle strengthening exercises, joint mobilization and muscle stretching to improve ROM, standing and walking exercises, pain and scar treatment, and other electromagnetic and heat treatments as necessary. Functional recovery was positively associated with rehabilitation intervention (OR=5.3; 95%CI 2.4-11.7), but it was negatively correlated with the immobilization duration (OR per 10-d increase=0.87; 95%CI 0.80-0.95), age (OR per 10-y increase=0.54; 95%CI 0.42-0.71), and depressive symptomatology (OR=0.21; 95%CI 0.06-0.72). Institution-based rehabilitation interventions delivered by physiotherapists, which included muscle strengthening exercises, joint mobilization and muscle stretching to improve ROM, standing and walking exercises, pain/scar treatment, and other electromagnetic and heat treatments as necessary. | ||||||||||||
| Rauch et al[ | Cross-sectional | Women | 18 | Earthquake | United States | Physical, psychological | Haiti Hospital Appeal (HHA) | 4-12 weeks | 3 days for 1 week with 4 weeks | One of the most important measures of physical rehabilitation was to provide wheelchairs and walkers in order to help patients walk. Amongst the most important rehabilitation activities, doing physical activity to prevent muscle deterioration, back massaging, changing positions to prevent bedsore and training for strengthening bladder were mentioned. For mental rehabilitation, mental support for injured people and their families, and providing psychological consultation meetings for them can prevent stress and anxiety disorders after the event. Results in this paper are related to functions and structures of spinal cord injury, which showed problems including complete impairments in defecation functions, bladder functions and muscle power functions. | ||||||||||||
| Tan et al[ | Case study | Children | No detail | Tsunami | India | Social, economical, psychological | Orphanages affected setting | Long term | No detail | The social, psychological rehabilitation and protection of children are main concerns of social organizations. Rehabilitation activates of UNICEF provides rice, milk and other basic rations including clean water and sanitation to the afflicted region through various programs with participation of countries. Other programs are: children vaccinated from fast-spreading diseases like measles, tetanus and gangrene. Another form of support for the orphans is to provide them with homes. The government and aid groups try to reunite the orphans with their next of kin, making sure that the people who claim the children are authentic relatives and not child traffickers. The creation of "Child-Friendly Spaces" (CFS) in camps and communities provides a platform from which children learn age-relevant competencies that help them cope with the risks and effects. In such an area where children meet other children, a sense of safety, structure and continuity enables them to find psychosocial and physical support, and encourage healthy development. | ||||||||||||
| Math et al[ | Cross-sectional | Children | 535 | Tsunami | India | Psychological | Camped, schooled | 0-72 | Each session lasted 90 to 120 minutes, and 10 to 20 participants were included in each | Psychological rehabilitation intervention for children used three methods: (1) mental health clinic; (2) art therapy; and (3) group discussions. Among art therapy, volunteers and teachers get the children from the relief camps and let them participate in drawing. Initially, participants were not given any theme for the drawings, but later they were asked to draw a picture of their place like village, school, home, playground, temple and environment. They were also asked to describe what they had drawn. This process helped the therapists screen out those who were severely affected by the disaster and these children were referred to psychiatrists in the mental health clinic. Among group discussions, students were asked to describe their experiences regarding the disaster and then the session focused on problems, concerns, and questions faced. Social welfare departments and Nicobar educated them on the need for mental health care for disaster survivors; the (NIMHANS) team contacted the relief camp organizers, school principals, teachers, leaders, and volunteers from the survivor groups to seek their cooperation and help. Intervention rehabilitation included identification of mental disorder symptoms, methods to normalize the daily activities of the children. Meeting counseling was considered until children express their feelings. | ||||||||||||
| Becker et al[ | Prospective cohort study | Women | 200 | Tsunami | India | Psychological | Affected setting | 4-12 weeks | 3 times per week for 2 h ours per session for 3 moths | Psychological rehabilitation intervention reported by this article for women's included: 10 trained community-level workers provided group sessions consisting of 10 participants, based on a train-a-trainer model; a 3-day experimental training program in psychological care (understanding and diagnosis, therapy techniques, stages of reactions and spectrum of care, needs assessments and referral, special needs of vulnerable groups of women, children, and disabled survivors) provided by the National Institute of Mental Health and Neurosciences professional team (psychiatrists, psychiatric social workers, nurses). Result showed 71% intervention group and 69% control group experienced 2 or more kinds of loss. Survey on intervention group showed 32% had symptoms of severe mental distress, and 22% moderate symptoms. In the control group it was reported 34% and 24% respectively. Significant decrease in total IES scores and subscale IES scores of avoidance, intrusion, and hyper vigilance, which indicated an improvement in symptoms for the psychosocial intervention group. | ||||||||||||
| Mallick et al[ | Cross-sectional | The disabled | 713 | Earthquake | Pakistan | Physical, psychological | Federal Ministry of Health, Institute of Medical Sciences, WHO Fund (UNICEF) | 4-12 weeks | 3 weeks | With the cooperation of International Handicapped NGO, a team consisting of 57 men and women passed the training courses on basic techniques and how to provide physical rehabilitation services to the spinal cord disabled and those who had undergone vertebral fixture operation to prevent creation of secondary complications. There was a specialized program dedicated to each of the injured individuals which was designed according to the type of injury and the degree of impaired person. Multi-strings approaches for physical rehabilitation were chosen. For enhancing the skills of semi-professional health service providing staff, instructions about increasing personal independence followed by spinal cord injuries has been translated and handed to employees. In addition, instructions for strengthening both patients and their families to adapt to physical limitations and increase personal independence by promoting the existed potentials were developed and handed to families and patients. Some principles about how to make wheelchairs and their adaptability with reconstruction programs were edited. Many patients got injured while they were trying to rescue their family members and most of them witnessed the death of their loved ones. International organizations have performed psychological rehabilitations to prevent negative mental responses in these individuals. | ||||||||||||
| Régnier et al[ | Case studies | Children, women, the elder | No detail | Tsunami | Indonesia | Economical | NGO | Long term | No detail | Rehabilitation economical actives after the tsunami in Indonesia is allocate 113 million euros for rehabilitation activities in Aceh by World Bank and private and governmental organizations of Nadu, Tamil, under the supervision of UNDP. A lot of economic rehabilitations intervention was conducted for buildings and shelters, and many infrastructure projects were completed by private organizations in Aceh. UNDP offered financial helps to reopen the cost line to help local people create small jobs, like fishing, and pay their life costs. After disaster, women had two types of indirect damage: job loss and damage to efficiency and family income | ||||||||||||
| Rathore et al[ | Case studies | The disabled | Estimated between 650 and 750 | Earthquake | Pakistan | Physical, physiological | Spinal unit at NIHD, Institute of Medical Sciences satellite hospital Mental Health Central Military Hospital Rawalpindi | 0-72 | No detail | Rehabilitation teams included: physical therapists, occupational therapists, orthopedics, and psychologists, allied health staffs, and other health care professionals around the world brought to Pakistan. Interventions rehabilitation by psychiatrists and psychologists, were aided by a large number of volunteers and social support groups. They were successful in alleviating the survivors' fears and detected their psychological needs. Patients were comforted and counseled to cope by using their religious teachings for inspiration. A religious organization named Al Huda, promoted Islamic knowledge among women of Pakistan. SCI rehabilitation teams provided useful education materials for patients. The physical rehabilitation interventions were provided by rehabilitation teams including: estimating and survey those who had spinal cord injury or amputation from an earthquake, and designing adaptive strategy with disabilities for these people; codification of appropriate policies for dealing with the disabilities caused by an earthquake; using comprehensive partnership to establish provider services organizations and rehabilitation programs; holding training courses for physical rehabilitation actives. | ||||||||||||
| Punani[ | Conference | The disabled | No detail | Earthquake | India | Physical | No detail | No detail | No detail | The most important physical rehabilitation measures for impaired people after disasters are: 1) determining proper dimensions and sizes for prostheses and providing enough physical rehabilitation services; all impaired persons need not only a fit prosthesis with the same size of the lost part, but also necessary trainings about how to properly use them; 2) physiotherapy: establishing physiotherapy centers in suitable positions at the disaster area through the help of NGOs, and private organizations is considered as one of the most influential parts of physical rehabilitation procedures; 3) establishing work therapy and rehabilitation centers: people get injured and disabled after earthquake. Sometimes, these people need help living their lives and paying costs. These centers can provide some facilities to recognize the remaining abilities of impaired persons and help them start or find a job. | ||||||||||||
| Authors | Study type | Vulnerable group | Sample size | Disaster type | Location | Type rehabilitation | Setting | Post disaster (phase) | Duration | Main concept | ||||||||||||
| Natural Man-made | ||||||||||||||||||||||
| Edgar et al[ | Case report | Women | 7 | No detail | Bombs exploded | .Indonesian | Physical | Royal Perth Hospital | 0-72 | 1 month, 6 months, 12 months | Rehabilitation activities after bomb explosion included: the injured people were transferred to hospitals in 3 groups via airplane. Surgical team conducted the necessary surgical measures for hospitalized patients within the first week: curing burns, splinting injured joints, temporal resting of affected limb and performing range of motion activities for muscles in order to prevent muscle deterioration. The injured individuals from bomb explosion were compared with normal unharmed people at the hospital within 1, 6 and 12 months after hospital discharge regarding 3 following factors such as shoulder active range of motion, grip strength, and the Burns Specific Health Scale. | |||||||||||
| Chiou-Tan et al[ | Retrospective chart analysis | Women | 133 | Hurricane | United States | Physical | Astrodome Clinic | 3-28 days | 1 week after hurricane Katri | After Hurricane Catharina, Astrodome medical clinic was established at the location of the incident within the first 12 hours. Through a period of 19 days, 11 245 patients were examined at this clinic. Except for the first day through which the clinic just conducted emergency medical services, physical rehabilitation activities provided helping tools such as wheelchairs and walkers, wound treatment materials, Baclofen pumps and pain killers and wheelchair user guide. Rehabilitations interventions included 14 subcategories as follows: foot and leg swelling, leg pain and cramps, headache, neck pain and back pain, skin wounds, fractures, humorous bone disease, neuropathy, leg musculoskeletal problems, musculoskeletal disorders, the brain stroke, bursitis and spinal cord injuries, musculoskeletal disorders and amputations, the most frequent of which were foot and leg swelling, leg pain and cramps, headache, neck pain and back pain. This study found that success of rehabilitation activities was the result of mutual cooperation between medical team of the clinic, supports for leading medical teams, volunteer doctors from Texas, and helps from private sector. | ||||||||||||
| Ni et al[ | Retrospective cohort study | Women | 154 | Earthquake | China | Social, physical | Hospital rehabilitation facilities | No detail | No detail | Comprehensive social and physical rehabilitation program included: therapeutic interventions, training and education, vocational and social rehabilitation. Result of this paper showed statistically significant differences in favor of the rehabilitation group in physical dysfunction (rehabilitation group 32.24%, control 67.76%). PTSD unadjusted data showed statistically significant differences in favor of the rehabilitation group and the controls. Being a woman, having average or above-average family income, having witnessed death, and fearfulness were risk factors for PTSD symptoms, 50 months after the earthquake. | ||||||||||||
| Randomized controlled trials studies analyses | ||||||||||||||||||||||
| Berger et al[ | Quasi-randomized controlled trial | Children | 166 | Tsunami | Sri Lanka | Physical, physiological | Temporary housing camps | Long term | First 3 months after the disaster | Physical and physiological rehabilitation activities in intervention group, included: teaching behavioral and cognitive skills, providing training materials, thinking practices, bio-energetic practices and techniques. The result of this paper showed that compared with the control group, PTSD severity, somatic complaints, functional problems and depression decreased in intervention groups after performing rehabilitation actives. | ||||||||||||
| Zhang et al[ | Quasi-experimental | Women | 331 | Earthquake | China | Physical, social | Non-governmental organizations, local health departments, and professional rehabilitation volunteers | Long term | 4 -10 moths for group (NHV-E) intervention, 16 moths for group intervention (VHV-L), 16 moths for group control | Physical rehabilitation program included: training in self-care and mobility activities; muscle strengthening and ROM, skin care management and education in bladder and bowel, traditional Chinese therapies. Social rehabilitation was included and empowerment was addressed via employment services and personal assistants. Result showed physical rehabilitation and physical functioning was increased in the NHV-L and NHV-E groups, but not in the control group after adjustment for sex, age, type of injury, and time to measurement. NHV-E improved BI scores by about 11.3 points at follow-up; NHV-L improved by 10.7 points. Significant effects were found in both the rehabilitation program and spontaneous recovery. The effect of NHV-E was marginally greater than that of NHV-L. | ||||||||||||
| Zang et al[ | Randomized control trial | The elder | 22 | Earthquake | China | Physical, psychological | Hospital and community rehabilitation facilities | 3-28 days | 4 therapy sessions (60-90 minutes) for 2 weeks with 2-4 daily between each session | Compared with wait list control group at post treatment, rehabilitation NET group had significant reductions in PTSD symptoms, IES-R avoidance, intrusion, and hyper arousal subscales anxiety and depression, HADS subscales, general mental stress, GHQ-28, and increased posttraumatic growth. NET in which the patient assisted by the therapist, constructed a detailed chronologic report of his/her own biography with a special focus on the traumatic experiences; the narrative was recorded by the counselor and corrected with each subsequent reading. The participants were encouraged to relive emotions while reporting the events. Rehabilitation program improved long-term functioning of Sichuan earthquake survivors with disabling injuries. | ||||||||||||
| 1 | Organisation WH, Time G. Earthquake disaster in Bam, Iran Preliminary indication of urgent requirements for those responding to the health needs of the affected population. 2003 (December). |
| 2 | Guha Sapir D, Vos F, Below R, Ponserre S. Annual Disaster Statistical Review 2010: The Numbers and Trends; Centre for Research on the Epidemiology of Disasters (CRED), Université catholique de Louvain: Brussels, Belgium, 2011; 41. |
| 3 |
Li XH, Hou SK, Zheng JC, Fan HJ, Song JQ. Post-disaster medical rescue strategy in tropical regions. World J Emerg Med. 2012; 3(1):23-8.
pmid: 25215034 |
| 4 |
Jha A, Basu R, Basu A. Studying policy changes in disaster management in india: a tale of two cyclones. Disaster Med Public Health Prep. 2016; 10(1):42-6.
pmid: 26477434 |
| 5 | National policy gudelie on vulnearable group in disaster published: may 2014. Available at: www.ndma.gov.pk/site/plans/gcc_policy |
| 6 | Kapucu N. Collaborative Governance and Disaster Recovery: The National Disaster Recovery Framework (NDRF) in the US. In: Disaster Recovery 2014; 41-59. |
| 7 | Punani B. Natural Disasters, Role of Disability Development Organizations. International Conference on Disasters & Disability; 28th & 29th January 2008; Shanta Memorial, Rehabilitation Centre, Bhubaneswar, Orissa; 62-64. |
| 8 |
Khatam A. The destruction of Bam and its reconstruction following the earthquake of December 2003. Cities. 2006; 23(6):462-4.
doi: 10.1016/j.cities.2006.08.008 |
| 9 |
Abdi K, Arab M, Rashidian A, Kamali M, Khankeh HR, Farahani FK. Exploring barriers of the health system to rehabilitation services for people with disabilities in Iran: A Qualitative Study. Electronic physician. 2015; 7(7):1476.
doi: 10.19082/1476 pmid: 26767101 |
| 10 |
Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009; 151(4):264-9, W64.
doi: 10.7326/0003-4819-151-4-200908180-00135 pmid: 19622511 |
| 11 | Critical Appraisal Skills Programme. 10 Questions to make sense of qualitative research [2006]. Available at: http://www.phru.nhs.uk/pages/phd/resources.htm. Accessed January 2008. |
| 12 | Critical Appraisal Skills Programme. CASP checklists. Available at: http://www.casp-tools-checklists/c18f8. Accessed September 20, 2014. |
| 13 |
Khankeh H, Nakhaei M, Masoumi G, Hosseini M, Parsa-Yekta Z, Kurland L, et al. Life recovery after disasters: a qualitative study in the Iranian context. Prehosp Disaster Med. 2013; 28(6):573-9.
doi: 10.1017/S1049023X1300900X pmid: 24300524 |
| 14 |
Adams V, Kaufman SR, Van Hattum T, Moody S. Aging disaster: mortality, vulnerability, and long-term recovery among Katrina survivors. Med Anthropol. 2011; 30(3):247-70.
doi: 10.1080/01459740.2011.560777 pmid: 21590581 |
| 15 |
Larson G, Drolet J, Samuel M. The role of self-help groups in post-tsunami rehabilitation. International Social Work. 2015; 58(5):732-42.
doi: 10.1177/0020872813477880 |
| 16 | Mansoor T, Yaqoob T. Psychological impact of disaster and rehabilitation of children in orphanages. J Asian Dev Stud. 2013; 2(3):6-17. |
| 17 |
Bazeghi F, Baradaran HR. The role of non-governmental organisations in the management of separated and unaccompanied children, following disasters in Iran. BMC Res Notes. 2010; 3:256.
doi: 10.1186/1756-0500-3-256 pmid: 20929548 |
| 18 | Huang Y, Wong H. Effects of social group work with survivors of the Wenchuan earthquake in a transitional community. Heal Soc Care Community. 2013; 21(3):327-37. |
| 19 | Jothi SP, Neelamalar M. The role of media in science and technology education,development and rehabilitation of women affected by the 2004 tsunami in the state of Tamilnadu. Science of Tsunami Hazards. 2011; 30(2):108-25. |
| 20 |
Becker SM. Psychosocial care for adult and child survivors of the 2004 tsunami disaster in India. Am J Public Health. 2006; 96(8):1397-8.
pmid: 16809599 |
| 21 |
Raissi GR. Earthquakes and rehabilitation needs: experiences from Bam, Iran. J Spinal Cord Med. 2007; 30(4):369-72.
doi: 10.1080/10790268.2007.11753954 pmid: 17853660 |
| 22 |
Li Y, Reinhardt JD, Gosney JE, Zhang X, Hu X, Chen S, et al. Evaluation of functional outcomes of physical rehabilitation and medical complications in spinal cord injury victims of the Sichuan earthquake. J Rehabil Med. 2012; 44(7):534-40.
doi: 10.2340/16501977-1005 pmid: 22674233 |
| 23 |
Xiao M, Li JA, Zhang X, Zhao ZE. Factors affecting functional outcome of Sichuan-earthquake survivors with tibial shaft fractures: a follow-up study. J Rehabil Med. 2011; 43(6):515-20.
pmid: 21533332 |
| 24 |
Rauch A, Baumberger M, Moise FG, von Elm E, Reinhardt JD. Rehabilitation needs assessment in persons with spinal cord injury following the 2010 earthquake in Haiti: a pilot study using an ICF-based tool. J Rehabil Med. 2011; 43(11):969-75.
pmid: 22031341 |
| 25 |
Tan NT. Impact of the Indian Ocean tsunami on the well-being of children. J Soc Work Disabil Rehabil. 2006; 5(3-4):43-56.
pmid: 17989010 |
| 26 |
Math SB, Tandon S, Girimaji SC, Benegal V, Kumar U, Hamza A, et al. Psychological impact of the tsunami on children and adolescents from the andaman and nicobar islands. Prim Care Companion J Clin Psychiatry. 2008; 10(1):31-7.
pmid: 18311419 |
| 27 |
Becker SM. Psychosocial care for women survivors of the tsunami disaster in India. Am J Public Health. 2009; 99(4):654-8.
doi: 10.2105/AJPH.2008.146571 pmid: 19150896 |
| 28 | Mallick M, Aurakzai JK, Bile KM, Ahmed N. Large-scale physical disabilities and their management in the aftermath of the 2005 earthquake in Pakistan. East Mediterr Health J. 2010; 16(Suppl):S98-105. |
| 29 |
Régnier P, Neri B, Scuteri S, Miniati S. From emergency relief to livelihood recovery: lessons learned from post-tsunami experiences in Indonesia and India. Disaster Prev Manag. 2008; 17(3):410-30.
doi: 10.1108/09653560810887329 |
| 30 |
Rathore FA, Farooq F, Muzammil S, New PW, Ahmad N, Haig AJ. Spinal cord injury management and rehabilitation: highlights and shortcomings from the 2005 earthquake in Pakistan. Arch Phys Med Rehabil. 2008; 89(3):579-85.
doi: 10.1016/j.apmr.2007.09.027 pmid: 18295642 |
| 31 | Punani B. Natural disasters, role of disability development organizations. Int Conf Disasters Disabil. 2008; 62-4. |
| 32 |
Edgar DW, Wood F, Goodwin-Walters A. First response, rehabilitation, and outcomes of hand and upper limb function: survivors of the Bali bombing disaster. A case series report. J Hand Ther. 2006; 19(3):283-97
doi: 10.1197/j.jht.2006.04.003 pmid: 16861128 |
| 33 |
Chiou-Tan FY, Bloodworth DM, Kass JS, Li X, Gavagan TF, Mattox K, et al. Physical medicine and rehabilitation conditions in the Astrodome clinic after hurricane Katrina. Am J Phys Med Rehabil. 2007; 86(9):762-9.
doi: 10.1097/PHM.0b013e31813e61cc pmid: 17710001 |
| 34 |
Ni J, Reinhardt JD, Zhang X, Xiao M, Li L, Jin H, et al. Dysfunction and post-traumatic stress disorder in fracture victims 50 months after the Sichuan earthquake. PLoS One. 2013; 8(10):e77535.
doi: 10.1371/journal.pone.0077535 pmid: 24204861 |
| 35 |
Berger R, Gelkopf M. School-based intervention for the treatment of tsunami-related distress in children: a quasi-randomized controlled trial. Psychother Psychosom. 2009; 78(6):364-71.
doi: 10.1159/000235976 pmid: 19738402 |
| 36 |
Zhang X, Reinhardt JD, Gosney JE, Li J. The NHV Rehabilitation Services Program improves long-term physical functioning in survivors of the 2008 Sichuan earthquake: a longitudinal quasi experiment. PLoS One. 2013; 8:e53995.
doi: 10.1371/journal.pone.0053995 pmid: 23308293 |
| 37 |
Zang Y, Hunt N, Cox T. A randomised controlled pilot study: the effectiveness of narrative exposure therapy with adult survivors of the Sichuan earthquake. BMC Psychiatry 2013; 13:41.
doi: 10.1186/1471-244X-13-41 pmid: 23363689 |
| 38 |
Gosney J, Reinhardt JD, Haig AJ, Li J. Developing post-disaster physical rehabilitation: role of the World Health Organization Liaison Sub-Committee on Rehabilitation Disaster Relief of the International Society of Physical and Rehabilitation Medicine. J Rehabil Med. 2011; 43(11):965-8.
pmid: 22031340 |
| 39 |
Talati S, Bhatia P, Kumar A, Gupta AK, Ojha CD. Strategic planning and designing of a hospital disaster manual in a tertiary care, teaching, research and referral institute in India. World J Emerg Med. 2014; 5(1):35-41.
pmid: 25215145 |
| 40 | World Health Organization. Community-based rehabilitation guidelines. Geneva: World Health Organization; 2010. |
| [1] | Amar Pujari, Deepa R Swamy, Rashmi Singh, Ritika Mukhija, Rohan Chawla, Pradeep Sharma. Ultrasonographic assessment of paediatric ocular emergencies: A tertiary eye hospital based observation [J]. World Journal of Emergency Medicine, 2018, 9(4): 272-275. |
| [2] | Vinej Somaraj, Rekha P Shenoy, Ganesh Shenoy Panchmal, Praveen S Jodalli, Laxminarayan Sonde, Ravichandra Karkal. Knowledge, attitude and anxiety pertaining to basic life support and medical emergencies among dental interns in Mangalore City, India [J]. World Journal of Emergency Medicine, 2017, 8(2): 131-135. |
| [3] | Deepak Geetaprasad Mishra, Tamorish Kole, Rahul Nagpal, Jeffery Paul Smith. A correlation analysis of Broselow™ Pediatric Emergency Tape-determined pediatric weight with actual pediatric weight in India [J]. World Journal of Emergency Medicine, 2016, 7(1): 40-43. |
| [4] | Ze-hua Dong, Bang-xu Yu, Yun-bo Sun, Wei Fang, Lei Li. Effects of early rehabilitation therapy on patients with mechanical ventilation [J]. World Journal of Emergency Medicine, 2014, 5(1): 48-52. |
| [5] | Xiang-hui Li, Shi-ke Hou, Jing-chen Zheng, Hao-jun Fan, Jian-qi Song. Post-disaster medical rescue strategy in tropical regions [J]. World Journal of Emergency Medicine, 2012, 3(1): 23-28. |
| [6] | Siu Ming Yang, Chor Man Lo. Transition to computed radiography: can emergency medicine doctors accurately predict the need of film printing to facilitate optimal patient care? [J]. World Journal of Emergency Medicine, 2011, 2(1): 33-37. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
