Posterior lamellar tarsorrhaphy in the early treatment of severe eyelid trauma/burns
|
Posterior lamellar tarsorrhaphy in the early treatment of severe eyelid trauma/burns |
| Neelam Pushker, Deepsekhar Das, Sujeeth Modaboyina, Pallavi Singh, Sahil Agrawal |
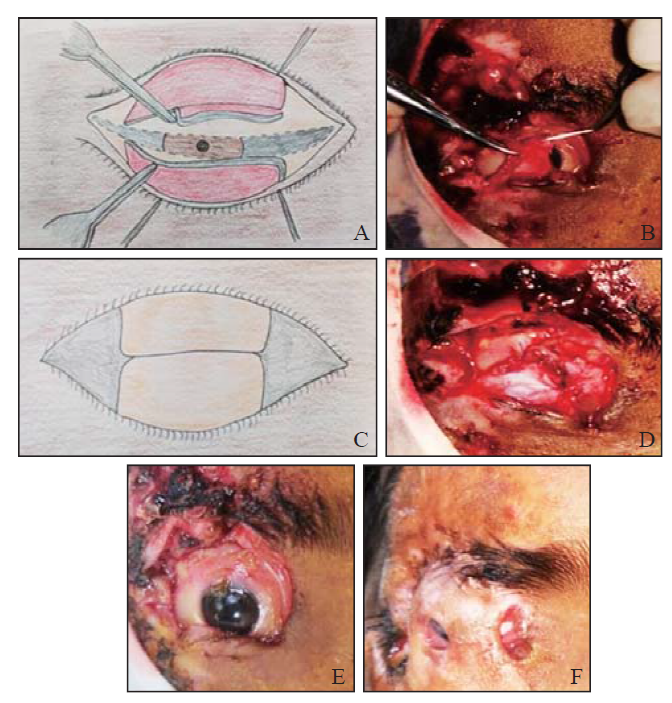
| Figure 1. Illustration of the surgical technique. A: sketch diagram shows advancement of posterior lamellae after splitting the eyelid margins and giving vertical lateral and medial cuts until borders of the tarsal plates in upper and lower eyelids, respectively; B: clinical photograph shows advancement of posterior lamellar flap of lower eyelid after giving medial and lateral vertical cuts till the lower tarsal border; C: sketch diagram shows the raw margins of both the posterior lamellae brought together and sutured using interrupted sutures; D: clinical photograph of same patients with upper and lower posterior lamellar flaps being advanced and sutured together using interrupted 6-0 polyglactin sutures; the traumatized/deficient anterior lamellae were left as such to heal with secondary intention; E: preoperative picture showing full thickness loss of upper and partial loss of lower lid with residual lid margin tissues, laterally with periorbital laceration wound with tissue loss and eschar formation; F: intact posterior lamellar tarsorrhaphy at 3-month follow-up in the same patient. |
|
|